

Research Article
Late Presentation of Cardiovascular Diseases: A Systematic Review and Meta-Analysis
- Meron Teklay Girmay 1**
- Fikremariam Melkeneh Alemayehu 2*
- Maru Yenehun Tsegaw 7
- Amanuel Tadesse Wondafrash 2
- Mikiyas Sharew Alemu 3*
- Tizita Kifle Negash 2*
- Haileselassie Asrat Kassa 4
- Mahlet Gebrehiwot Tolera 8*
- Yonatan Tsetadirgachew Legesse 5*
- Eyoel Ameha Sebsibe 6
- Eden Fanta Amajo 2
- Million Ahmed Muhe 2
- Amanuel Aklilu Alemu 2
- Abera Girma Beyena 5
- Bikiltu Belissa Gobosho 2
- Solomon Endale Dagnachew 2
1Department of Medicine, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia.
2Department of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia.
3Department of Medicine, Myungsung Medical College, Addis Ababa, Ethiopia.
4Department of Medicine, College of Medicine and Health Sciences, Injibara University, Injibara, Ethiopia.
5Department of Medicine, Asella College of Health Sciences, Arsi University, Asella, Oromia, Ethiopia.
6Department of Medicine, Santé Medical College, Addis Ababa, Ethiopia.
7Department of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia.
8Department of Medicine, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia.
*Corresponding Author: Fikremariam Melkeneh Alemayehu, Mikiyas Sharew Alemu, Tizita Kifle Negash, or Mahlet Gebrehiwot Tolera and Yonatan Tsetadirgachew Legesse.
Citation: Girmay MT, Alemayehu FM, Tsegaw MY, Alemu MS, Negash TK, et al. (2026). Late Presentation of Cardiovascular Diseases: A Systematic Review and Meta-Analysis, Journal of Clinical Cardiology and Cardiology Research, BioRes Scientia Publishers. 5(1):1-8. DOI: 10.59657/2837-4673.brs.26.053
Copyright: © 2026 Meron Teklay Girmay, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 15, 2026 | Accepted: June 03, 2026 | Published: June 08, 2026
Abstract
Introduction: Cardiovascular diseases remain the leading cause of morbidity and mortality worldwide. Despite advances in diagnostic and therapeutic strategies, a considerable proportion of patients continue to present late in the course of disease, which is associated with poor clinical outcomes and increased mortality. So, this review is aimed at assessing the prevalence of late Presentation of Cardiovascular Diseases.
Materials and Methods: PubMed, Google Scholar, Scopus, Web of Science, and Google databases were searched for this analysis. The methodological quality was assessed using the Newcastle-Ottawa Scale. An inverse variance-weighted random-effects model meta-analysis was performed to estimate the pooled late-stage presentation. The I2 test statistic was used to check between-study heterogeneity, and the Egger's regression statistical test was used to check publication bias. A p-value of less than 0.05 is used to declare statistical significance.
Results: The included studies had good methodological quality. Most studies were conducted in Asia. The magnitude of late presentation of cardiovascular diseases was found to be 58.2% (95% CI: 38.2-78.0). The highest prevalence of late Presentation of cardiovascular Diseases is 72.7% (95% CI: 52.0-93.5), which was seen in Africa region, and the lowest is 70.2% (95% CI: 55.9-85.6) was seen in Asia region.
Conclusion: Despite of late presentation is associated with increased risk of complications, including irreversible organ damage, higher mortality, and greater healthcare costs late presentation remains a persistent challenge in this study. Therefore, addressing delays in presentation is essential for improving patient outcomes and reducing the global burden of cardiovascular diseases.
Keywords: late presentation; cardiovascular diseases; review; global; delayed diagnosis; delayed hospital presentation
Introduction
Cardiovascular diseases (CVDs) continue to be the leading cause of morbidity and mortality worldwide, accounting for approximately 18.9 million deaths each year and nearly 32% of all global deaths. Conditions such as coronary artery disease, heart failure, and stroke contribute substantially to this burden, especially in low- and middle-income countries where access to early detection and appropriate treatment remains limited. Although major advances have been achieved in cardiovascular diagnosis and management, many patients still seek medical care at advanced stages of disease, leading to poorer clinical outcomes and increased mortality rates [1-6].
Late presentation of cardiovascular disease, commonly defined as hospital arrival more than six hours after symptom onset, represents a major public health concern associated with increased morbidity and mortality. Delays may arise from several patient-related factors, including poor awareness of symptoms, socioeconomic challenges, and cultural beliefs, as well as healthcare system-related barriers such as inadequate access to medical services, delayed diagnosis, and inefficient referral pathways. Previous studies have demonstrated that delayed presentation is particularly frequent among patients with acute cardiovascular conditions, especially myocardial infarction [7-11].
Research has further shown that delayed medical attention substantially elevates the risk of severe complications, including irreversible myocardial injury, heart failure, long-term disability, and sudden cardiac death [12-14]. As cardiovascular diseases remain one of the major causes of premature mortality and disability globally, with an increasing incidence worldwide [15], understanding the prevalence and contributing factors of late presentation is essential for designing effective interventions that promote early diagnosis and timely treatment. Therefore, this systematic review and meta-analysis aim to synthesize the existing evidence regarding the prevalence of late presentation among patients with cardiovascular diseases.
Materials and Methods
Study Design and Search Strategy
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16]. The review question was developed using the POCC framework: Population: all age groups; Outcome: prevalence/proportion; Condition: late presentation; and Context: global setting involving observational studies. A comprehensive literature search strategy was performed in three stages. First, the advanced PubMed search engine was used to identify relevant studies through Medical Subject Headings (MeSH) terms and free-text searches using Boolean operators (“AND” and “OR”). Titles, abstracts, and indexing terms of relevant articles were also reviewed to refine the search process. Second, additional electronic databases, including Google Scholar, Scopus, Web of Science, and Google, were searched to identify eligible studies.
The search strategy included combinations of the following terms: “prevalence” OR “proportion” OR “epidemiology” AND “cardiovascular disease” OR “congestive heart failure” OR “CHD” OR “congenital heart disease” AND “diagnosis” OR “medical care” OR “seek care” AND “global.” Finally, the reference lists of all eligible articles were manually screened to identify additional relevant studies. Only studies published in the English language up to April 2026 were included in the review. Search filters, including language of publication, were applied during the selection process.
Eligibility Criteria
This study included all observational studies reporting the prevalence late Presentation of Cardiovascular Diseases without a limitation of study period. Both published and unpublished studies conducted in English were considered. Whereas reviews, short reports, and case reports were excluded from this study.
Data Extraction and Outcome
After completion of the literature search, data extraction was conducted independently by pairs of reviewers using a standardised data extraction format. The extracted data were recorded in a Microsoft Excel 2013 spreadsheet and included the following information: author’s name, year of publication, study design, sample size, study setting, and prevalence of late presentation of cardiovascular diseases. The primary outcome of this systematic review and meta-analysis was to determine the pooled prevalence of late presentation among patients with cardiovascular diseases.
Quality Assessment of Studies
The methodological quality of the included studies was assessed using the modified Newcastle–Ottawa Scale (NOS) for cross-sectional studies. The scale evaluates studies based on three domains: selection, comparability, and outcome assessment, with a maximum score of 10 points [17]. Studies scoring five or more points on the NOS were considered to have acceptable methodological quality and were included in the analysis [18]. Quality assessment was performed independently by the authors, and any disagreements were resolved through discussion and consensus after thorough review of the studies by all authors.
Effect Measures
The effect measure used in this study was the proportion of patients with late presentation of cardiovascular diseases, which was used to estimate the pooled prevalence across the included studies.
Data Analysis and Synthesis Methods
After extraction, the eligible study data were exported to Stata version 14 software for statistical analysis. A random-effects model was employed to estimate the pooled prevalence due to anticipated heterogeneity among the included studies, which could arise from differences in study settings, participant characteristics, and variations in risk factors related to the outcome. Between-study heterogeneity was assessed using Higgins’ I² statistic. An I² value of less than 50% was considered low heterogeneity, 50-75% moderate heterogeneity, and >75% high heterogeneity [19]. Subgroup analysis was conducted based on geographic region to explore potential sources of heterogeneity. Publication bias was evaluated using funnel plot visualization and Egger’s regression test. In addition, sensitivity analyses were performed to determine the robustness and stability of the pooled estimates.
Results
Study Selection
The search strategy retrieved a total of 1402 published articles. After removing duplicates using reference management software, 1175 articles remained. Following further screening, 383 articles were assessed for eligibility. Out of these, 371 articles were excluded because they didn’t meet the inclusion criteria. Finally, twelve studies were included in the analysis (Figure 1).
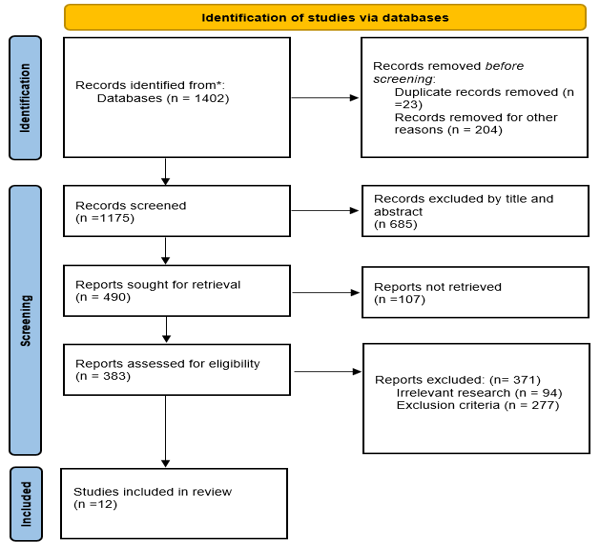
Figure 1: PRISMA Flow Diagram of Study Selection for the Global Prevalence of Late Presentation of Cardiovascular Diseases.
Characteristics of The Studies
All twelve [20-31] had a total of 6900 participants and had good methodological quality. The final sample size ranges from 187 [27]- 1991 [25]. Most studies were conducted in Asia. The magnitude of Cardiovascular Lesions ranged from 3.8 [43] – 89.8 [42] (Table 1).
Table 1: Characteristics of the included studies in the systematic review and meta-analysis.
| Authors Name | Publication Year | Study Area | Study Design | Sample Size | Prevalence with 95% CI |
| Chaka TE | 2025 | Addis Ababa | Cross-sectional | 228 | 53.1(46.6-59.5) |
| Rashid U | 2016 | Pakistan | Cross- sectional | 354 | 85.1(81.3-88.8) |
| Iqbal SH, | 2021 | Pakistan | Cross-sectional | 265 | 79.6(74.7-84.4) |
| Murni IK, | 2021 | Indonesia | Cohort | 838 | 60.8(57.4-64.1) |
| Ng’eno M, | 2023 | Kenya | Cross-sectional | 411 | 60.6(55.8-65.3) |
| Jadhav H, | 2025 | India | Cross-sectional | 1991 | 85.1(83.5-86.6) |
| Hurisa T, | 2022 | Addis Ababa | Cross-sectional | 216 | 95.4(92.6-98.1) |
| Birlie TA, | 2024 | Debre Tabor | Cross-sectional | 187 | 81.6(76.0-87.1) |
| Massin MM, | 2006 | Belgium | Cross-sectional | 744 | 8.9(6.8-10.9) |
| Liberman RF, | 2014 | USA | Cross-sectional | 916 | 13.8(11.5-16.0) |
| Zahid Z, | 2022 | Pakistan | Cross-sectional | 500 | 38(33.7-42.2) |
| Kumari V, | 2023 | Pakistan | Cross-sectional | 250 | 72.8(67.2-78.3) |
Prevalence of Late Presentation of Cardiovascular Diseases
The pooled proportion of Late Presentation of Cardiovascular Diseases was found to be 61.2% (95% CI: 40.3-82.1) with a heterogeneity index of 99.8%, with a P-value of less than 0.001(Figure 2). Due to a significant in the Egger test with a p-value of 0.003. Trim and fill analysis was conducted then the pooled prevalence was found to be 58.2% (95% CI: 38.2-78.0).
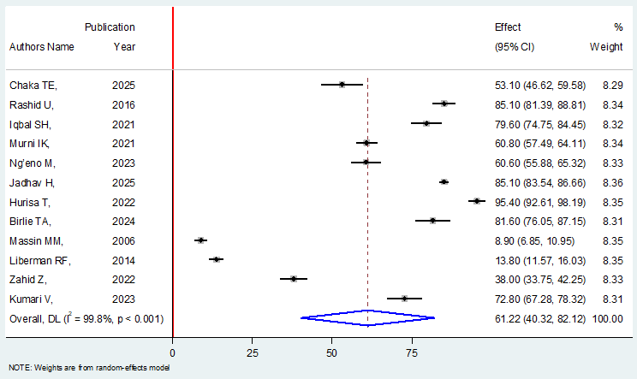
Figure 2: Forest Plot Showing the Global Pooled Prevalence of Late Presentation of Cardiovascular Diseases.
Sub-Group Analysis
The subgroup analysis was conducted based on the region of the studies conducted. The highest prevalence of late Presentation of cardiovascular Diseases is 72.7% (95% CI: 52.0- 93.5, I2 = 98.8%) was seen in Africa region, and the lowest is 70. 2% (95% CI: 55.9.-85.6, I2 = 98.8%) was seen in Asia region (Figure 3).
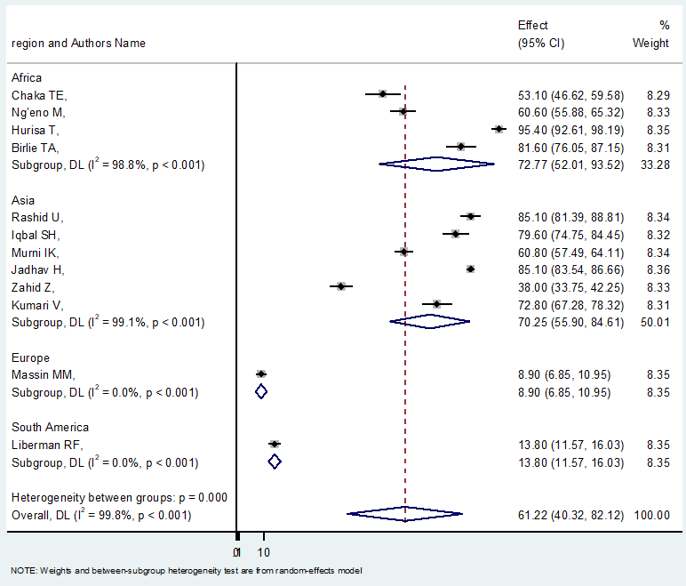
Figure 3: Subgroup Analysis of the Global Pooled Prevalence of Late Presentation of Cardiovascular Diseases by Region.
Meta-Regression and Publication Bias
The heterogeneity index value indicated that the studies were quite varied. Therefore, meta-regression was conducted using year of publication and sample size as covariates. The analysis showed that sample size and publication year didn’t have a significant effect on heterogeneity between studies, with a P- value of 0.504 and 0.091, respectively. Publication bias was assessed using a funnel plot and the Egger regression test with a significance threshold of less than 0.05. Statistical evidence of publication bias was observed. The funnel plot appears asymmetrical in the distribution, and the Egger test yielded a statistically significant result with a coefficient value of 0.021and P-value of 0.003 (Figure 4). As a result, trim and fill analysis was conducted, and then the funnel plot appeared nearly symmetrical (Figure 5).
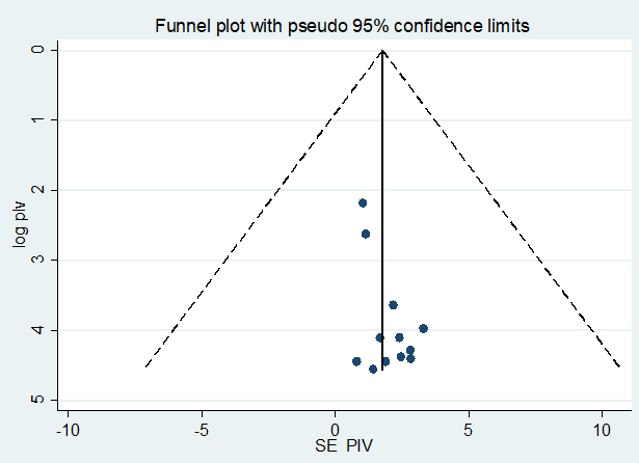
Figure 4: Funnel Plot Assessing Publication Bias Among Included Studies.
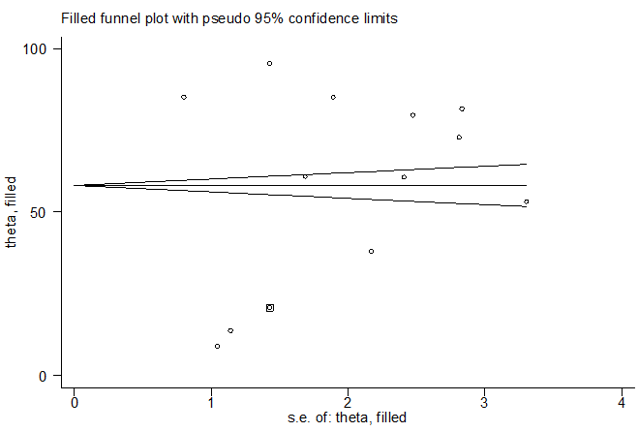
Figure 5: Funnel Plot After Trim-and-Fill Analysis for Publication B.
Sensitivity Analysis
Sensitivity analysis was performed to determine how various sources of uncertainty contribute to the overall uncertainty among the studies, but the results indicated that uncertainty has an insignificant influence on pooled prevalence of late presentation of cardiovascular disease (Figure 6).
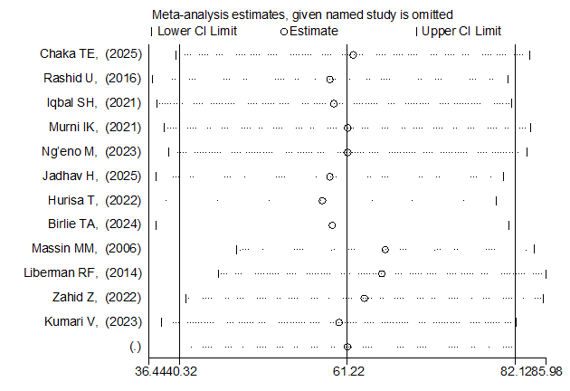
Figure 6: Sensitivity Analysis of the Global Pooled Prevalence of Late Presentation of Cardiovascular Diseases.
Discussion
The shift from physically demanding to sedentary jobs, along with the current consumerism and technology-driven culture that is related to longer work hours, longer commutes, and less leisure time for recreational activities, results a significant increase in the rates of CVD [32]. Early diagnosis of complex heart diseases leads to improved preoperative morbidity and mortality [33,34].
The present study shown that the pooled prevalence of late presentation of cardiovascular diseases was 58.2% (95% CI: 38.2-78.0), indicating that more than half of patients with cardiovascular conditions seek medical care after a significant delay. This finding indicates a substantial gap in timely healthcare utilization and is consistent with previous studies that have reported high rates of delayed presentation [35-37].
The subgroup analysis demonstrated regional variation, with the highest prevalence of late presentation observed in Africa (72.7%) and relatively lower prevalence in Asia (70.2%). Although both regions show high proportions, the slightly higher burden in Africa may reflect differences in healthcare access, socioeconomic status, and awareness levels.
The high heterogeneity observed across studies (I² = 98.8%) suggests considerable variability in the reported prevalence of late presentation. This variation may be explained by differences in study design, demographic characteristics, healthcare delivery systems, cultural beliefs, health-seeking behaviors, and levels of symptom awareness differ across populations and may influence the timing of presentation.
Delayed care in cardiovascular diseases, particularly in conditions like coronary artery disease, is associated with increased morbidity, mortality, and poor outcomes. Evidence suggests that early recognition and prompt treatment significantly reduce complications such as heart failure and sudden cardiac death.
Conclusion
Despite of late presentation is associated with increased risk of complications, including irreversible organ damage, higher mortality, and greater healthcare costs: late presentation remains a persistent challenge in this study. Therefore, addressing delays in presentation is essential for improving patient outcomes and reducing the global burden of cardiovascular diseases.
Limitation of The Study
This systematic review and meta-analysis faced limitations. First, the presence of significant heterogeneity and publication bias means that the results should be interpreted with caution. Secondly, we encountered difficulties in comparing our results due to the absence of regional and worldwide systematic reviews and meta-analyses.
Declarations
Ethics Approval and Consent to Participant
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
The data analyzed during the current systematic review and meta-analysis is fully available with reasonable request.
Competing Interests
all the authors declare that they have no competing interests
Funding
The authors received no specific funding for this work
Acknowledgment
We would like to thank all authors of studies included in this systematic review and meta-analysis.
References
- WHO, (2025). Cardiovascular Diseases.
Publisher | Google Scholor - British heart foundation Global Cardiovascular Disease Factsheet
Publisher | Google Scholor - Roth, G. A., Mensah, G. A., Johnson, C. O., Addolorato, G., Ammirati, E., et al. (2020). Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update from The GBD 2019 Study. Journal of The American College of Cardiology, 76(25):2982-3021.
Publisher | Google Scholor - de Oliveira Laterza Ribeiro, M., Correia, V. M., Herling de Oliveira, L. L., Soares, P. R., Scudeler, T. L. (2023). Evolving Diagnostic and Management Advances in Coronary Heart Disease. Life, 13(4):951.
Publisher | Google Scholor - Regan, J. A., Laitner, M. H., Dzau, V. J. (2025). A Crossroads in Cardiovascular Medicine: Progress and Barriers to Impact. Circulation, 152(16):1166-1173.
Publisher | Google Scholor - Ting, H. H., Bradley, E. H., Wang, Y., Lichtman, J. H., Nallamothu, B. K., et al. (2008). Factors Associated with Longer Time from Symptom Onset to Hospital Presentation for Patients With ST-Elevation Myocardial Infarction. Archives of Internal Medicine, 168(9):959-968.
Publisher | Google Scholor - Taghaddosi, M., Dianati, M., Bidgoli, J. F. G., Bahonaran, J. (2010). Delay and Its Related Factors in Seeking Treatment in Patients with Acute Myocardial Infarction. ARYA Atherosclerosis, 6(1):35.
Publisher | Google Scholor - Farshidi, H., Rahimi, S., Abdi, A., Salehi, S., Madani, A. (2013). Factors Associated with Pre-Hospital Delay in Patients with Acute Myocardial Infarction. Iranian Red Crescent Medical Journal, 15(4):312.
Publisher | Google Scholor - Politi, R. E., Mills, P. D., Zubkoff, L., Neily, J. (2022). Delays in Diagnosis, Treatment, And Surgery: Root Causes, Actions Taken, and Recommendations for Healthcare Improvement. Journal of Patient Safety, 18(7):e1061-e1066.
Publisher | Google Scholor - Barwise, A., Leppin, A., Dong, Y., Huang, C., Pinevich, Y., et al. (2021). What Contributes to Diagnostic Error or Delay? A Qualitative Exploration Across Diverse Acute Care Settings in The United States. Journal of Patient Safety, 17(4):239-248.
Publisher | Google Scholor - Dziewierz, A., Zdzierak, B., Wańha, W., Luca, G. D., Rakowski, T. (2025). The Irreversible March of Time: Ischemic Delay and Impact on Outcomes in ST-Segment Elevation Myocardial Infarction. Journal of Cardiovascular Development and Disease, 12(12):474.
Publisher | Google Scholor - Karatza, A. A., Fouzas, S., Gkentzi, D., Kostopoulou, E., Loukopoulou, C., et al. (2025). Missed or Delayed Diagnosis of Heart Disease by The General Pediatrician. Children, 12(3):366.
Publisher | Google Scholor - Eckersley, L., Sadler, L., Parry, E., Finucane, K., Gentles, T. L. (2016). Timing of Diagnosis Affects Mortality in Critical Congenital Heart Disease. Archives of Disease in Childhood, 101(6):516-520.
Publisher | Google Scholor - Vos, A., Van der Wal, A. C., Teeuw, A. H., Bras, J., et al. (2018). Cardiovascular Causes of Sudden Unexpected Death in Children and Adolescents (0-17 Years) A Nationwide Autopsy Study in The Netherlands. Netherlands Heart Journal, 26(10):500-505.
Publisher | Google Scholor - Flora, G. D., Nayak, M. K. (2019). A Brief Review of Cardiovascular Diseases, Associated Risk Factors and Current Treatment Regimes. Current Pharmaceutical Design, 25(38):4063-4084.
Publisher | Google Scholor - Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., et al. (2021). The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ, 372.
Publisher | Google Scholor - Modesti, P. A., Reboldi, G., Cappuccio, F. P., Agyemang, C., Remuzzi, G., et al. (2016). Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PloS One, 11(1):e0147601.
Publisher | Google Scholor - Herzog, R., Álvarez-Pasquin, M. J., Díaz, C., Del Barrio, J. L., Estrada, J. M., et al. (2013). Are Healthcare Workers’ Intentions to Vaccinate Related to Their Knowledge, Beliefs and Attitudes? A Systematic Review. BMC Public Health, 13(1):154.
Publisher | Google Scholor - Higgins, J. P., Thompson, S. G., Deeks, J. J., Altman, D. G. (2003). Measuring Inconsistency in Meta-Analyses. BMJ, 327(7414):557-560.
Publisher | Google Scholor - Chaka, T. E., Ali, H. A., Tadele, H. (2025). Delayed Diagnosis of Congenital Heart Diseases and Associated Factors in The Largest Tertiary Hospital in Ethiopia. Cardiovascular Diagnosis and Therapy, 15(5):955-965.
Publisher | Google Scholor - Rashid, U., Qureshi, A. U., Hyder, S. N., Sadiq, M. (2016). Pattern of Congenital Heart Disease in A Developing Country Tertiary Care Center: Factors Associated with Delayed Diagnosis. Annals of Pediatric Cardiology, 9(3):210-215.
Publisher | Google Scholor - Iqbal, S. H. A. H. I. D., Saidullah, S. H. A. H. A. B., Ahmed, R. I., Khan, M. A. A., Ahmed, N. I. S. A. R., et al. (2021). Factors Contributing to Delayed Diagnosis of Congenital Heart Disease in Pediatric Population. Age (Years), 2(184):69-64.
Publisher | Google Scholor - Murni, I. K., Wirawan, M. T., Patmasari, L., Sativa, E. R., Arafuri, N., et al. (2021). Delayed Diagnosis in Children with Congenital Heart Disease: A Mixed-Method Study. BMC Pediatrics, 21(1):191.
Publisher | Google Scholor - Ng’eno, M., Del-rossi, S. Q., Gachara, N., Kihurani, I., Yonga, G. (2023). Late Diagnosis of CHD and Its Associated Factors in Kenya: An Analytic Cross-Sectional Study. Cardiology in The Young, 33(10):1902-1908.
Publisher | Google Scholor - Jadhav, H., Weekey, P., Dalwai, K., Deshpande, V. (2025). Bridging the Diagnostic Gap: A Retrospective Study on Missed and late Diagnoses of Congenital Heart Disease in Neonates and Children. Journal of Heart Valve Disease, 30:41-46.
Publisher | Google Scholor - Hurisa T, Megersa H, Tsegaye T. (2022). Delayed in Diagnosis of Congenital Heart Disease and Associated Factors Among Pediatric Patients in Cardiac Center Addis Ababa, Ethiopia, 2021 G.C. American Journal of Health Research, 10(3):51-62.
Publisher | Google Scholor - Birlie, T. A., Amare, A. T., Agegn, S. B., Yirga, G. K., Bantie, B., et al. (2024). Treatment Seeking Delay and Associated Factors in Adult Heart Failure Patients Admitted to Debre Tabor Comprehensive Specialized Hospital, North West, Ethiopia. Heliyon, 10(1).
Publisher | Google Scholor - Massin, M. M., Dessy, H. (2006). Delayed Recognition of Congenital Heart Disease. Postgraduate Medical Journal, 82(969):468-470.
Publisher | Google Scholor - Liberman, R. F., Getz, K. D., Lin, A. E., Higgins, C. A., Sekhavat, S., et al. (2014). Delayed Diagnosis of Critical Congenital Heart Defects: Trends and Associated Factors. Pediatrics, 134(2):e373-e381.
Publisher | Google Scholor - Zahid, Z., Khan, H. S., Mazhar, Z., Anam, M. (2022). Factors and Morbidities Associated with The Delayed Diagnosis of Congenital Heart Disease in Children Under 5. Esculapio - JSIMS [Internet]. 18(4):422-426.
Publisher | Google Scholor - Kumari, V., Khan, M. A., Chand, R., Ahsan, A. K., Khokhar, R. A., et al. (2023). Factors Linked with The Delayed Diagnosis of Congenital Heart Diseases. A Single Center Experience from A Tertiary Care Hospital of Pakistan. The Professional Medical Journal, 30(10):1288-1292.
Publisher | Google Scholor - Lopez, E. O., Ballard, B. D., Jan, A. (2023). Cardiovascular Disease. In StatPearls [Internet]. StatPearls Publishing.
Publisher | Google Scholor - Chakraborty, A., Gorla, S. R., Swaminathan, S. (2018). Impact of Prenatal Diagnosis of Complex Congenital Heart Disease on Neonatal and Infant Morbidity and Mortality. Prenatal Diagnosis, 38(12):958-963.
Publisher | Google Scholor - Bonnet, D. (2021). Impacts of Prenatal Diagnosis of Congenital Heart Diseases on Outcomes. Translational Pediatrics, 10(8):2241.
Publisher | Google Scholor - Mol, K. A., Rahel, B. M., Meeder, J. G., van Casteren, B. C., Doevendans, P. A., et al. (2016). Delays in The Treatment of Patients with Acute Coronary Syndrome: Focus on Pre-Hospital Delays and Non-ST-Elevated Myocardial Infarction. International Journal of Cardiology, 221:1061-1066.
Publisher | Google Scholor - Kontsevaya, A. V., Kononets, E. N., Goryachkin, E. A. (2019). Delayed Help-Seeking for Emergency Medical Care of Patients with Acute Coronary Syndrome/Myocardial Infarction: Review of Studies. Journal of Cardiology, 98.
Publisher | Google Scholor - Viana, M., Laszczyńska, O., Araújo, C., Borges, A., Barros, V., et al. (2020). Patient and System Delays in The Treatment of Acute Coronary Syndrome. Revista Portuguesa de Cardiologia, 39(3):123-131.
Publisher | Google Scholor























