

Research Article
Iridescent Skin Disorders in RH+Z-F1 Cases: A New Approach to testing Genetic Abnormalities and Intradermal Muscoskeletal Abnormalites of the Skin and Dermis
1 Oak Ridge Aerospace Institute DOE, DPO Outlying Islands.
2 Lofton Epigenetics Laboratories, DPO Outlying Islands, Jan Mayen Svalbaard.
3 Fleet Ecology Institute on Metallurgic Studies, DPO Outlying Island.
*Corresponding Author: Dr V Lunde Dadon MD PhD, Oak Ridge Aerospace Institute DOE, DPO Outlying Islands.
Citation: V Lunde Dadon, Wolfsson, Dadiane L. (2025). Iridescent Skin Disorders in RH+Z-F1 Cases: A New Approach to testing Genetic Abnormalities and Intradermal Muscoskeletal Abnormalites of the Skin and Dermis, Clinical Case Reports and Studies, BioRes Scientia Publishers. 10(4):1-4. DOI: 10.59657/2837-2565.brs.25.267
Copyright: © 2025 V Lunde Dadon, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 30, 2025 | Accepted: July 14, 2025 | Published: July 21, 2025
Abstract
We have sanction research into Skin Disorder in this article involving Dermal Skin Grafts and Muscoskeletal Abnormalities. In article you will be presented with Case studiesduring the latent phases of the Skin Disorders. Certain areas of our research are inhabitable to inactive prognosis or deactivated insurance cases for non-coverage due to Genetic Abnormalities.
Keywords: : iridescent skin; genetic abnormalities of skin; sports medicine disease of skin; dermis injury; muscoloskeletal abnormality due to skin disorder; species RH+Z-F1 taxonomy; ICD-11 diseases of skin; dermatological disease; epidermolysis bullosa
Introduction
We have sanction research into Skin Disorder in this article involving Dermal Skin Grafts and Muscoskeletal Abnormalities. In article you will be presented with Case studies during the latent phases of the Skin Disorders. Certain areas of our research are inhabitable to inactive prognosis or deactivated insurance cases for non-coverage due to Genetic Abnormalities. We will educate you on a list of Iridescent Skin Disorder, and set aside one to discuss in this Article and Book series. The list will advance your knowledge of visible Iridescent Skin Disorders, which is important in the field of Immunology, Dermatology, and Epidemiology, and Endocronology. After reviewing the list, we will set aside a Dermatological Disease and discuss the classification in depth with indexed ICD-11 codes assigned. Taxonomy of the species with manifestations are the RH+Z-F1 Taxonomy of Species in Zoology Classifications. This species was discovered in Europe, America’s, and Asia, Middle East/Africa. Next, we discuss Epidermolysis Bullosa. The RH+Z-F1 is a Humane Classifcation for New Approaches to Research.
Figure 1: Here we illustrate Microscopic Cell Bioremediation from our Labs, to show the species manifestation and skin cell biology through Microscopic Sciences. Certain Skin Grafts we utilized for Iridescent Skin Disorders are manufactured in the laboratory.
The Research involves Humane-Animal Contact, reviews vaccines such as TDAP, Vaxelis, other prescribing rituals used in Dermatology and Disease. The dermatitis diagnosis is also related to Sports Medicine and Physiotherapy, and discussions on Genetics and abnormality of Skin and muscloskeletal underlying Anomalies, and manifestations due to Dermatopic Infection, spread of the Dermatological Disease, and its manifestations into signs and symptoms related to General Medicine. Some infections to the skin have caused the gluing of fingers, toes, and mouth, and genital/vaginal/penisal areas to be affected. Muscle movements can be affected due to the abnormal dermis contact with the Muscloskeletal System and causing physiological pain, paralysis, gluing, and contracting and flexing of muscles due to dermis injury or disease.

Figure 2: Here we illustrate methods used in research to reach the Nerve Cells, Muscoskeletal and Dermis;we collect samples for testing and research such as Vaccines, we advise not to perform these procedures outside of Laboratory Protocals. This method we use in our Medical Case was dry needling, and microscopic skin cell adhesion to dry slides. We have used the list of iridescent skin disorders, but we focus here on Epidermolysis Bullosa (Skin Sample by Dry Needling).
Methodology of Applied Research Prognosis and Testing
Laboratory Methodology: We have assigned a medical case evaluation and methodology here, to approach this prognosis and further testing with Scientific Deductive Reasoning and Prognosis.
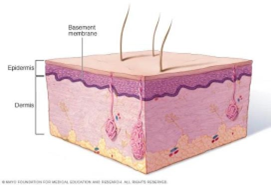
Figure 3: Here we illustrate the Layer of the Skin as it has its foundation to the Muscoskeletal System at the base. The layers of the Skin are labelled here and shown here for reference.
We have completed the first series of interpretation (briefly) of patients with the disease assigned a Medical Case Research into Epidermolysis Bullosa. Our Method of Approach to complete the understanding of the Disease in order to move towards, with Prognosis and Testing. We have gathered a list of Iridescent Skin Disorders, and now we have assigned one skin disorder to our method of deductive reasoning into a Scientific Analysis and further Medical Investigations.
The disorder known as Epidermolysis bullosa (ep-ih-dur-MOL-uh-sis buhl-LOE-sah) is a rare condition that causes fragile, blistering skin. The blisters may appear in response to minor injury, even from heat, rubbing or scratching. In severe cases, the blisters may occur inside the body, such as the lining of the mouth or stomach. Epidermolysis bullosa is inherited, and it usually shows up in infants or young children. Some people don't develop symptoms until they're teens or young adults. Epidermolysis bullosa has no cure, but mild forms may improve with age. Treatment focuses on caring for blisters and preventing new ones. The list of other Iridescent Skin Disorders are Chromhidrosis, Dermatographia, Lichen Planus, Scars, Melanoma, Aneurysmal atypical fibroxanthoma, Hemosiderotic dermotofibroma, Basal Cell Carcinoma, Kaposi Sarcoma, Intra Muscular Stasis Dermatitis (Dermal), Skin Graft Carcinoma, Skin Burn Dermatitis, Angiokeratoma.

Figure 4: Here, the patient presents with a Atypical Epidermolysis Bullosa, and has reached the internal cavities of the dermis, and muscoloskeletal system, we performed a dry needle sampling to illustrate our method towards research and testing (objective approach).
Medical Analysis of Disease Manifestations in Experimental Case
The Disease Epidermolysis has significant manifestations into the overall “body” systems. It also is inherited, and Genetics play an important role in reporting and classification of the skin disease. It has other signs and symptoms that can be categorized as General Medicine or Internal Medicine disorders. As this disease spreads it can cause paralysis to the muscles, muscle spasms, fever, and secondary infections. This can be classified under Infectious Disease. The infectious Disease Genetically-determined epidermal disease EB43 Epidermolysis Bullosa acquisita (EC30-EC3Z) (KA07.Y), EBA (epidermolysis bullose acquisita), Epidermolysis bullosa acquisita Brunsting-Perry type. Epidermolysis bullosa is caused by an inherited gene. You may inherit the disease gene from one parent who has the disease (autosomal dominant inheritance) or from both parents (autosomal recessive inheritance).

Figure 5: Here we illustrate the Ribosomal DNA, DNA, and transcriptase, transfer into the Skin Cell DNA, and the Cycle of Elimination of membranes, or antibodies.
The skin is made up of an outer layer (epidermis) and an underlying layer (dermis). The area where the layers meet is called the basement membrane. The types of epidermolysis bullosa are mainly defined by which layers separate and form blisters. The skin injury might be brought on by a minor injury, bump or nothing at all. Further Medical Analysis categorized the Skin Disorder into three parts.
The main types of epidermolysis bullosa are:
• Epidermolysis bullosa simplex: This is the most common type. It's brought on by heat and friction and develops in the outer layer of skin. It mainly affects the palms and feet. The blisters heal without scarring.
• Junctional epidermolysis bullosa: This type may be severe, with blisters beginning in infancy. A baby with this condition may develop a hoarse-sounding cry from continual blistering and scarring of the vocal cords.
• Dystrophic epidermolysis bullosa: This type is related to a flaw in the gene that helps produce a protein that glues the skin layers together. If this protein is missing or doesn't function, the layers of the skin won't join properly. It can cause skin that looks thin. Diseased mucous membranes can cause constipation and make it hard to eat, removal of the gallbladder is a common secondary infection because it doesn’t respond to metabolic functions after the disease has manifested into the gastrointestinal organs.
• Kindler syndrome: This type tends to cause blisters in multiple layers and so can look very different from person to person. The blisters tend to show up in infancy or early childhood. It increases sun sensitivity and causes skin to look thin, mottled and wrinkly.
Conclusion
To summarize the Iridescent Skin Disorders, and links to Genetics and DNA with Muscloskeletal Functions, we remove all questions into why the immune system doesn’t respond to certain skin conditions as rapidly as we prognosis. In the Modern Day we have to continue research into Advancing Studies into Infectious Disease and Skin Disorders, especially Epidermolysis Bullosa, and diagnose accordingly based on Taxonomy of Zoological Disease, and ICD-11. There are vaccines available such as TDAP, and Vaxelis, TDAP can only assist if there’s an autoimmune response to a pathogen, Vaxelis is for Humane- Animal Cases to provide seroimmunogenecity to the environmental conditions that may or may not cause a serious Skin Disorder to manifest.
Laboratories
• Lofton Infectious Disease Institute for Research and Development, Jan Mayen Svalbaard, FIS, RFI
• Ocean Bio_ Med Pharmaceuticals and Bio_RAD Testing Labs, Oak Ridge, FIS, RFI
• Premier MD Laboratories with Apollo MED Microscopic Labs and Research Center, FIS, RFI
Declarations
Conflict of Interest
We don’t have an open access to this journal, it was publishedby a private laboratory and there’s fee’s for purchasing the journal in a professional environment.
Acknowledgement
Dr V Lunde Dadon PhD, Dr Wolfsson PhD, Dr L Dadiane MD.
Acknowledgement to Laboratories
Oak Harbor’s Ridge Laboratories, Lofton Epigenetics Corporation GmBH, Research Institute Arctic Regulation Commission Amsterdam, Axial University, Aerospace International Nuclear Research Institute, WIPO/Patents Brisbane Australia, Ocean Canteen, Ocean Bio_Med Corporation, Biomedical and Biopharmaceuticals Futopia Autodesk, Island HealthGroup, NordX Biopharmaceuticals previously Noridian Laboratories, Organ and Tissue Banking Laboratories L.P.
References
- Dadin, L. (2009). ICD-11 classification of disease: Medical dossier on CPT advantages into crosswalks.
Publisher | Google Scholor - Journal of the American Academy of Dermatology. (2022). Integrating skin disorders into clinical practice and research. JAAD,91(6):1189–1198.
Publisher | Google Scholor - Elsevier. (2022). Clinical trials and skin disorders: The example of skin tumors. Dermatology, 238:180–184.
Publisher | Google Scholor - Reddy, V. D., & Myers, B. S. (n.d.). Disparities in dermatology: A reflection.
Publisher | Google Scholor - Lyon, & Lundbeck. (2014). Research techniques made simple: Cutaneous colorimetry (iridescent): A reliable technique for objective skin color measurements. JAAD Case Reports, 4:1019–1054.
Publisher | Google Scholor























