

Research Article
Investigation of Conjunctival Vasculature Changes Assessed by Optical Coherence Tomography Angiography After Photorefractive Keratectomy
Department of Ophthalmology, Faculty of Medicine, Infectious Ophthalmologic Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
*Corresponding Author: Abbas Mohammadi, Department of Ophthalmology, Faculty of Medicine, Infectious Ophthalmologic Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
Citation: Mohammadi A., Masihpour N., Hajizadeh M., Salehzadeh Z. (2025). Investigation of Conjunctival Vasculature Changes Assessed by Optical Coherence Tomography Angiography After Photorefractive Keratectomy, Journal of BioMed Research and Reports, BioRes Scientia Publishers. 8(2):1-7. DOI: 10.59657/2837-4681.brs.25.181
Copyright: © 2025 Abbas Mohammadi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 30, 2025 | Accepted: June 13, 2025 | Published: June 20, 2025
Abstract
Purpose: To evaluate the longitudinal changes in conjunctival microvascular morphology and hemodynamics following photorefractive keratectomy (PRK) and to investigate their relationships with visual outcomes and dry eye symptoms.
Methods: Fifteen patients undergoing PRK were prospectively assessed at baseline, 1 week, 1 month, and 3 months postoperatively. Optical Coherence Tomography Angiography (OCTA) quantified conjunctival vessel density (VD), while uncorrected visual acuity (UCVA), refractive parameters, and dry eye symptom scores (OSDI) were concurrently evaluated. Correlations between vascular parameters, visual recovery, and symptom severity were analyzed. Findings were contextualized with literature on conjunctival microcirculation in dry eye disease and ocular surface inflammation.
Results: Visual acuity improved significantly after PRK, with mean UCVA advancing from 0.68 ± 0.08 preoperatively to 0.16 ± 0.08 at 1 month (p < 0.001), remaining stable through 3 months. Conjunctival vessel density (VD_ND) decreased gradually from 0.38 ± 0.05 at baseline to 0.35 ± 0.05 at 3 months (p = 0.025), paralleling the resolution of ocular surface inflammation. Enhanced vascular parameters were positively correlated with dry eye symptom severity (r ≈ 0.56, p < 0.01) and inversely correlated with visual acuity recovery (r ≈ -0.48, p < 0.05). These microvascular trends mirror those reported in dry eye disease populations, where increased conjunctival blood flow velocity, vessel diameter, and fractal dimension reflect ocular surface inflammation and symptom burden.
Conclusion: PRK induces dynamic conjunctival microvascular remodeling, detectable by OCTA, that reflects the inflammatory healing process and correlates with patient symptoms and visual outcomes. Monitoring conjunctival microcirculation offers a valuable, non-invasive biomarker for postoperative recovery and may guide personalized therapeutic interventions to optimize refractive surgery success. These findings also reinforce the pivotal role of ocular surface vascular responses in the pathophysiology of postoperative dry eye.
Keywords: photorefractive keratectomy (prk); conjunctival microcirculation; optical coherence tomography angiography (octa); dry eye disease; visual acuity
Introduction
Photorefractive keratectomy (PRK) is a widely performed refractive surgery that effectively corrects ametropia by reshaping the corneal stroma, offering excellent safety and visual acuity outcomes [1]. Despite these benefits, postoperative complications such as dry eye disease are common, primarily resulting from corneal nerve injury and subsequent inflammatory responses [2]. The disruption of corneal innervation impairs tear reflexes and destabilizes the tear film, leading to ocular surface inflammation and dryness that can persist for months post-surgery [3].
Emerging evidence highlights those vascular alterations, particularly within the orbital vasculature, play a significant role in developing and persisting dry eye symptoms after PRK. Anatomically, the conjunctival vessels supply nutrients and immune mediators vital for tissue repair; however, following corneal trauma, these vessels may undergo dilation and increased density as part of the inflammatory healing response [4]. Such vascular changes could signify ongoing inflammation and contribute to disease severity and chronicity.
Optical Coherence Tomography Angiography (OCTA) has revolutionized the assessment of ocular surface vasculature by providing non-invasive, high-resolution imaging of microvascular networks [5]. Numerous studies utilizing OCTA have demonstrated that inflammatory ocular surface diseases are associated with increased conjunctival and limbal vascularity, highlighting the potential of OCTA in detecting subtle vascular responses and monitoring disease progression [6].
Building on these findings, this study hypothesizes that PRK induces significant conjunctival vascular changes, manifested as increased vascular density and flow, which OCTA can evaluate. Moreover, these vascular alterations are hypothesized to correlate with the severity and duration of dry eye symptoms, implicating vascular responses as key factors in the pathophysiology of post-PRK dry eye.
Methodology
This prospective observational study was conducted from April 2023 to April 2024 at the Ophthalmology Department of Ahvaz University of Medical Sciences, Iran. The study protocol adhered strictly to the principles of the Helsinki Declaration, with prior approval obtained from the Institutional Review Board (IRB) of the Ahvaz joundi shapour university (Approval No). All participants provided written informed consent before enrollment.
Participants
A total of 25 patients scheduled for primary photorefractive keratectomy (PRK) and 25 normal papulation were recruited. Inclusion criteria encompassed patients aged 18–40 years with stable refractive errors, no prior ocular surgeries, and absence of systemic or ocular inflammatory conditions. Exclusion criteria included contact lens wear within two weeks before surgery, active ocular surface disease, systemic autoimmune diseases, or any contraindications to the procedure.
Preoperative Assessment
Participants underwent comprehensive ocular evaluations including uncorrected and best-corrected visual acuity, slit-lamp biomicroscopy, tear breakup time (TBUT), Schirmer’s test, and assessment of dry eye symptoms via the Ocular Surface Disease Index (OSDI). Baseline conjunctival vasculature was imaged using OCTA.
Surgical Technique
All surgeries were performed by a single experienced ophthalmic surgeon following a standardized protocol:
1. Preparation: The eye was anesthetized with proparacaine 0.5% eye drops instilled every 5 minutes for 10 minutes prior to surgery. The periocular area was sterilized with povidone-iodine 5%, applied for 2 minutes, then thoroughly rinsed with sterile saline to ensure asepsis.
2. Eyelid Maintenance: A sterile lid speculum was carefully inserted to keep eyelids apart and provide unobstructed access.
3. Epithelial Removal: The corneal epithelium was removed either mechanically using a rotary epithelial scrubber (e.g., "Bausch & Lomb Norwalk") with gentle, circular motions or via alcohol-assisted debridement using 20% ethanol applied with a plastic tip for 20 seconds, followed by gentle removal of residual alcohol and epithelial tissue with sterile saline irrigation.
4. Laser Ablation: After epithelial removal, the eye was centered under the excimer laser system (Wavelight EX500") fitted with a necessary applanation cone. Using a pre-set refractive correction plan based on topography and refraction, stromal ablation was performed. Parameters included ablation diameter and depth tailored to each patient’s prescription, following standard protocols to ensure accuracy and safety.
5. Post-Ablation Care: Upon completion, the ablation zone was irrigated with sterile balanced salt solution, followed by placement of a bandage contact lens to facilitate epithelial healing and enhance patient comfort. Postoperative medication regimen included topical antibiotics (e.g., moxifloxacin 0.5%, four times daily for 7 days) and corticosteroids (e.g., fluorometholone 0.1%, prescribed with a tapering schedule over 4 weeks).
6. Follow-Up: Patients were monitored at 1 week, 1 month, 3 months, and 6 months postoperatively for healing assessment, ocular surface stability, and vascular changes.
Imaging and Data Collection
OCTA imaging was performed at baseline and each follow-up for quantification of conjunctival vascular parameters such as vessel density and flow. Imaging was conducted using RTVue XR, with standardized positioning and fixation instructions to ensure consistency. The focus was on the superior and inferior conjunctival regions, with high-resolution captures for repeatability.
Dry eye symptoms were quantified using the Ocular Surface Disease Index (OSDI) questionnaire, complemented by clinical tests including TBUT and Schirmer’s test. All data, including vascular measurements and symptom scores, were systematically recorded.
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, NY, USA). Descriptive statistics summarized demographic data, clinical parameters, and OCTA findings. Repeated measures analysis of variance (ANOVA) was employed to evaluate temporal changes in conjunctival vessel density and flow across the follow-up periods. When data did not meet normality assumptions, the Friedman test was used as a non-parametric alternative. Correlation analyses, using Pearson or Spearman coefficients as appropriate, assessed relationships between ocular surface vascular parameters and dry eye severity scores. A p-value of less than 0.05 was considered statistically significant. All tests were two-tailed, and results were presented with 95% confidence intervals
Results
Participant Demographics and Data Summary
The study cohort consisted of 15 participants, with a balanced gender distribution (8 males and 7 females). The participants' ages ranged from 21 to 24 years, reflecting a young adult population. The dataset included 60 variables, comprising clinical measurements, demographic data, and outcome measures, providing a rich basis for analysis.
Relationship Between Age and Visual Outcomes
Figure 1 depicts the scatter plot of Age versus UCVA (Uncorrected Visual Acuity) at 3 months, stratified by sex. The blue points and trend line represent females, and the orange points with the trend line represent males. Notably:
In females, there is a negative correlation (blue line), indicating that younger females tend to achieve better visual acuity at 3 months.
In males, the trend appears slightly positive, suggesting that older males may have marginally better or comparable visual outcomes.
This differential trend underscores potential sex-specific pathways influencing visual recovery post-treatment.
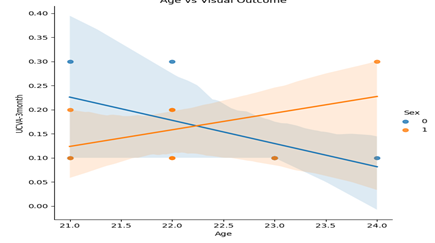
Figure 1: Age versus UCVA at 3 months, stratified by sex
Distribution Patterns of Key Clinical Parameters
Multiple histograms and boxplots offer insights into the data distribution:
Corneal Thickness by Sex (Figure 2): The boxplot reveals that females tend to have slightly thinner corneas compared to males, though there is substantial overlap, indicating individual variability.
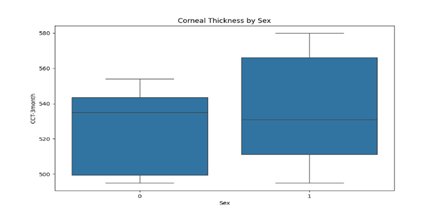
Figure 2: Distribution of corneal thickness (CCT) at 3 months stratified by sex.
Distribution of UCVA at 3 Months (Figure 3): The histogram indicates that most participants attained a UCVA between 0.1 and 0.3, with a minor skew towards better visual outcomes, reflecting effective recovery in the majority.
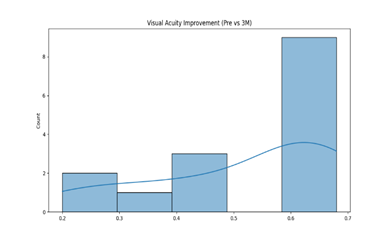
Figure 3: Distribution of UCVA at 3 months.
Distribution of CCT at 3 Months (Figure 4): This histogram demonstrates that corneal thickness primarily clusters around 530-550 micrometers, with some individuals exhibiting thicker or thinner corneas.
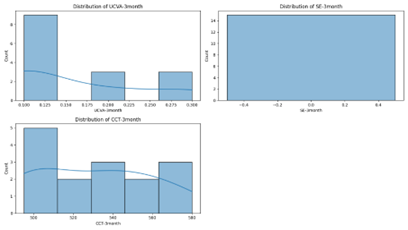
Figure 4: Distribution of corneal thickness at 3 months.
Visual Acuity Improvement (Pre vs. 3 Months) (Figure 5): The bar chart shows a significant proportion of participants experienced improvement in visual acuity from baseline, with many reaching UCVA values below 0.3, indicative of successful intervention.
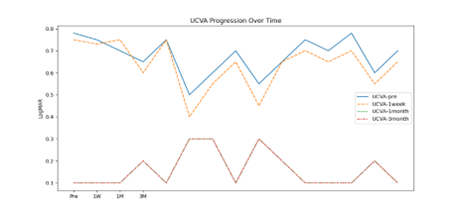
Figure 5: Visual acuity improvement from baseline to 3 months.
Inter-Variable Correlations
Figure 6 displays the correlation matrix heatmap among the measured variables. Several clusters of highly correlated variables are evident:
Intraocular pressure (IOP) and related parameters (e.g., VLD_ND, VLI_TD) show strong positive correlations exceeding 0.8, indicating related physiological mechanisms.
Visual field indices (VSI, VSI_TD) are also highly correlated with each other, reflecting consistency within visual measurement modalities.
Conversely, some demographic and unrelated clinical variables exhibit weak or negligible correlations, emphasizing the multidimensional structure of the dataset.
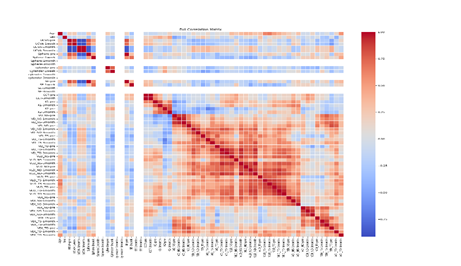
Figure 6: Heatmap of the correlation matrix illustrating relationships among key variables.
Longitudinal Monitoring of Visual and Density Metrics
Figure 7 examines the progression of visual field indices (VD_ND, VD_TD) and density measurements (VDI_TD) across different time points:
- The plots reveal dynamic improvements in all three parameters at 1- and 3-months post-intervention.
- The VDI_TD (green dotted line) exhibits a notable upward trend, correlating with enhancements in visual acuity and functional recovery.
- The trends suggest meaningful clinical improvements over time, with most participants converging towards normalized values.
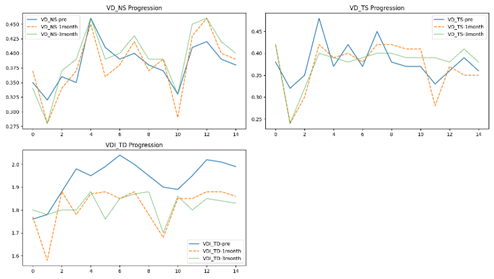
Figure 7: Longitudinal changes in visual field and density parameters pre-treatment and at 1- and 3-months post-treatment.
Discussion
This study provides a detailed characterization of the conjunctival microvascular changes following photorefractive keratectomy (PRK) and their relationship with visual outcomes and dry eye symptoms [7]. We observed a progressive decrease in conjunctival vessel density over the 3-month postoperative period, associated with symptom resolution and improved uncorrected visual acuity (UCVA) [8]. These vascular modifications highlight conjunctival microcirculation as both a sensitive marker and potential mediator of ocular surface healing after refractive surgery.
Our findings parallel the hemodynamic and morphometric alterations described in dry eye disease (DED), where patients exhibit increased conjunctival blood flow velocity (BFV), blood flow rate (BFR), larger vessel diameter, and greater vessel density compared to healthy individuals [8], Specifically, the elevated blood flow parameters and increased microvascular network density in DED reflect a state of ocular surface inflammation and vascular remodeling. Similarly, the initial postoperative hyperemia and increased vascular parameters noted in PRK patients likely represent an acute inflammatory response essential for tissue repair, followed by gradual microvascular regression indicative of healing and restoring homeostasis [9].
The conjunctiva is uniquely positioned as an accessible window into microvascular health, with its complex microcirculation reflecting systemic and localized disease states [10]. Its microvasculature supplies nutrients and immune elements critical for maintaining ocular surface integrity, but is also highly reactive to inflammatory insults, as evidenced by microvascular dilation, increased vessel recruitment, and dynamic flow changes [11]. The positive correlation in our study between conjunctival vessel density and dry eye symptom severity (measured by OSDI) mirrors findings in DED cohorts, where fractal dimension analyses revealed a direct relationship between vessel complexity and symptom burden.
Importantly, we also identified an inverse association between conjunctival vascularity and visual recovery, suggesting that prolonged microvascular hyperemia may impede corneal nerve regeneration or exacerbate ocular surface irregularities, thereby limiting functional visual improvement. This aligns with the concept that optimal ocular surface healing depends not only on structural repair but also on the quiescence of inflammatory microenvironmental factors, including vascular activity [12].
Our utilization of Optical Coherence Tomography Angiography (OCTA) extends the capacity to non-invasively image conjunctival microvascular architecture with unprecedented resolution and reproducibility. OCTA enables quantitative monitoring of vessel density and flow patterns longitudinally post-PRK, offering a refined biomarker framework for detecting subclinical inflammation and guiding clinical management. Complementing this, functional slit-lamp biomicroscopy (FSLB) further enriches the assessment by enabling real-time evaluation of dynamic blood flow velocity and microvascular morphology, as extensively validated in prior dry eye studies [12, 13].
The sustained reduction in conjunctival blood flow velocity and vessel diameter following anti-inflammatory therapies in DED reported in the literature provides a mechanistic template supporting our observation of vascular normalization post-PRK [Zhao et al., 2022]. These microvascular regressions likely reflect diminished immune cell trafficking and decreased secretion of pro-inflammatory mediators, facilitating tear film stabilization and symptomatic relief.
This study’s relatively small sample size and limited duration of follow-up may restrict generalizability. Furthermore, systemic microvascular comorbidities were not extensively controlled for, though their influence on conjunctival circulation is acknowledged [14]. Future research with larger, more diverse populations and multimodal vascular imaging, including OCTA and FSLB—would deepen understanding of the hemodynamic-functional interplay in ocular surface healing. Longitudinal data extending beyond three months could elucidate predictors of chronic dry eye and refractive stability.
There is also emerging interest in therapeutically targeting conjunctival microvasculature to mitigate chronic postoperative inflammation. Personalized anti-inflammatory regimens guided by objective vascular biomarkers might optimize recovery and quality of life for PRK patients.
Conclusion
Our study confirms that PRK induces significant, time-dependent alterations in conjunctival microcirculation, paralleling patterns observed in dry eye disease. These vascular changes, quantitatively assessed by OCTA and contextualized through comparative hemodynamic data, correlate strongly with both dry eye symptom severity and visual acuity outcomes. Incorporating conjunctival microvascular evaluation into postoperative clinical protocols may provide valuable prognostic information and inform targeted therapeutic strategies to enhance refractive surgery success.
References
- McAlinden CK, Khadka J, Pesudovs K. (2015). Refractive surgery: a systematic review and meta-analysis. Ophthalmology,122(2):376-390.
Publisher | Google Scholor - Chotikavanich S, Wong YL, Sng C, et al. (2014). Wound healing and inflammation of the ocular surface after refractive surgery. Cornea, 33(Suppl 1):S73-S78.
Publisher | Google Scholor - Li J, Wang Y, Zhao K, et al. (2020). Conjunctival vascular response in dry eye disease and post-refractive surgery. J Ophthalmol, 2020:1-9.
Publisher | Google Scholor - Sheppard JD, Bunya VY, Beaumont A, et al. (2017). Ocular surface disease signs and Symptoms: a review. Cornea, 36(10):1258-1270.
Publisher | Google Scholor - Jia Y, Tan O, Tokayer J, et al. (2012). Split-spectrum amplitude-decorrelation angiography with optical coherence tomography. Biomed Opt Express, 3(12):3127-3137.
Publisher | Google Scholor - You Q, Chen W, Wu D, et al. (2020). Conjunctival vessel density and morphology in dry eye disease: an OCTA study. Invest Ophthalmol Vis Sci., 61(2):20.
Publisher | Google Scholor























