

Review Article
Integrating Mental Health Services into Maternal Health Programmes in Sub-Saharan Africa: A Systematic Review
- Onyekachi Darlington Bennette Ojiaku *
Independent Researcher, Lagos State, Nigeria.
*Corresponding Author: Onyekachi Darlington Bennette Ojiaku, Independent Researcher, Lagos State, Nigeria.
Citation: O.D.B. Ojiaku. (2025). Integrating Mental Health Services into Maternal Health Programmes in Sub-Saharan Africa: A Systematic Review, Clinical Case Reports and Studies, BioRes Scientia Publishers. 10(4):1-13. DOI: 10.59657/2837-2565.brs.25.268
Copyright: © 2025 Onyekachi Darlington Bennette Ojiaku, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 01, 2025 | Accepted: July 15, 2025 | Published: July 22, 2025
Abstract
This systematic review evaluates the integration of mental health services into maternal health programmes in Sub-Saharan Africa (SSA) from 2010 to 2025, guided by the Ubuntu Wellness Web framework, which organises findings across individual, family, community, and health system threads. Maternal mental health disorders, affecting 20–30% of mothers in SSA, are often neglected despite their impact on maternal and child outcomes. Using PRISMA 2020 guidelines, 10 primary studies from Nigeria, Uganda, Ethiopia, Malawi, South Africa, Gambia, Gabon, Senegal, Kenya, and Zambia were synthesised to assess effectiveness, barriers, and facilitators of integration. Narrative synthesis was employed to analyse heterogeneous study designs, including quantitative, qualitative, and mixed-methods research. Findings indicate moderate effectiveness, with screening tools (e.g., Edinburgh Postnatal Depression Scale, Patient Health Questionnaire-9) detecting depression in 12–18% of mothers, task-shared counselling reducing symptoms by 30–42%, and peer-support models improving resilience and care-seeking by 40–50%, particularly among adolescent mothers. The Text4Life mHealth intervention enhanced access, though no studies reported artificial intelligence (AI) or electronic medical records (EMR), highlighting a digital gap. Barriers included stigma, limited community health worker training, gender norms, and connectivity issues, while facilitators encompassed validated tools, task sharing, and community approval. The Ubuntu Wellness Web underscores the need for culturally tailored, collaborative solutions. An envisioned mHealth app leveraging AI and EMR could bridge the digital divide, enhancing scalability. Recommendations include funding CHW training, integrating screening into routine care, and expanding peer-support programmes. This review provides a foundation for strengthening maternal mental health care in SSA, aligning with Ubuntu’s collective ethos to support healthier mothers and communities.
Keywords: EMR; ubuntu; health programmes
Introduction
Overview
This systematic review explores the integration of mental health services into maternal health programmes in Sub-Saharan Africa (SSA) from 2010 to 2025, employing the Ubuntu Wellness Web framework to organise findings across individual, family, community, and health system threads. Maternal mental health disorders, such as depression and anxiety, represent a significant yet often neglected challenge in SSA, where maternal health programmes primarily focus on physical health outcomes. By synthesising evidence on the effectiveness, barriers, and facilitators of integration, this review aims to inform policy and practice, proposing culturally relevant and digitally innovative solutions, including an envisioned mobile health (mHealth) application leveraging artificial intelligence (AI) and electronic medical records (EMR) to enhance maternal mental health care.
Burden of Maternal Mental Health in SSA
Maternal mental health disorders, including postpartum depression and anxiety, affect a substantial proportion of women in SSA, with significant implications for their wellbeing and that of their families. Studies estimate that 20–30% of mothers in SSA experience depression or anxiety, a prevalence notably higher than the 10–15% reported in high-income countries [1,2]. In Nigeria, for instance, approximately 22% of postpartum women report depressive symptoms, while in Uganda, adolescent mothers face elevated risks of anxiety due to social and economic pressures [3,4]. These conditions disrupt the individual thread of the Ubuntu Wellness Web, as untreated mental health issues impair maternal functioning, hinder child bonding, and increase risks of developmental delays, underscoring the urgent need for integrated care within existing maternal health frameworks.
Untreated maternal mental health disorders extend their impact beyond the individual, straining family and community dynamics. Research indicates that maternal depression is associated with reduced breastfeeding rates and poor infant bonding, contributing to adverse child health outcomes [5]. In SSA, economic pressures exacerbate these challenges, as untreated mental disorders reduce maternal productivity, placing additional burdens on families [6]. These effects weaken the family and community threads of the Ubuntu Wellness Web, as mothers’ roles as caregivers and community contributors are compromised, highlighting the interconnected nature of maternal mental health and communal wellbeing.
SSA health systems face significant constraints in addressing maternal mental health, with limited resources and prioritisation of physical health. Many SSA countries have fewer than one psychiatrist per million people, severely limiting access to specialised care [7]. Maternal health programmes often focus on reducing mortality from physical conditions like haemorrhage, sidelining mental health services despite their critical impact [8]. This resource scarcity within the health system thread necessitates integration strategies that leverage existing maternal care platforms to deliver mental health support efficiently, aligning with the collective ethos of Ubuntu.
The Ubuntu Wellness Web Framework
The Ubuntu Wellness Web provides a culturally grounded framework for integrating mental health services into maternal health programmes, rooted in the African philosophy of Ubuntu, which emphasises interconnectedness through the principle “I am because we are” [9]. This framework organises care across four threads: individual (for example, screening and counselling), family (for example, partner support), community (for example, peer groups), and health system (for example, task sharing). Unlike Western models that prioritise individual therapy, the Ubuntu Wellness Web embraces SSA’s communal values, ensuring interventions resonate with local contexts. Strengthening one thread, such as community support, reinforces others, fostering holistic maternal wellbeing and aligning with SSA’s cultural strengths.
Importance of Integration
Integrating mental health services into maternal health programmes maximises reach and efficiency in SSA’s resource-constrained settings. Maternal health programmes provide regular touchpoints, such as prenatal and postnatal visits, which are ideal for delivering screening and counselling services [10]. Task-sharing with community health workers (CHWs) has proven effective in low-resource settings, leveraging existing workforce capacity [11]. This approach strengthens the health system thread, offering a sustainable model for delivering mental health care within existing infrastructure, consistent with Ubuntu’s focus on collective responsibility.
Community-based approaches further enhance integration by addressing cultural barriers such as stigma. Evidence suggests that community interventions, such as peer-support groups, improve care-seeking behaviours in SSA by fostering acceptance and reducing misconceptions about mental health [12]. These strategies strengthen the community thread, aligning with Ubuntu values and making integrated interventions more effective and culturally acceptable across diverse SSA contexts.
Literature Gaps and Opportunities
Research on integrating mental health services into SSA maternal health programmes remains limited, particularly for vulnerable groups like adolescents and rural populations. Most studies focus on standalone mental health interventions, such as hospital-based therapy, with few exploring integrations within routine maternal care [13]. Adolescents, who face heightened mental health risks, and rural mothers, often distant from health facilities, are underrepresented in existing literature [14]. This gap highlights the need for studies on culturally tailored integration strategies, which this review addresses through the Ubuntu Wellness Web framework, amplifying SSA voices and informing context-specific programme design.
Digital health interventions, including AI and EMR, are underexplored in SSA maternal mental health care. While some studies report mHealth use, there is a notable absence of AI or EMR applications, indicating a significant digital gap [15]. This presents an opportunity for innovation, such as the envisioned mHealth app, to enhance access and scalability, particularly in the health system thread, by leveraging technology to overcome resource constraints.
Rationale
Integrating mental health services into maternal health programmes is essential for achieving holistic care in SSA, where maternal mental health significantly impacts child health and community well-being [5,7]. By embedding mental health support within existing maternal care platforms, this approach leverages SSA’s limited resources effectively, aligning with the Ubuntu Wellness Web’s emphasis on interconnected, community-driven solutions to strengthen maternal health outcomes across all threads.
Aims and Objectives
Aim: To explore the integration of mental health services into maternal health programmes in SSA, using the Ubuntu Wellness Web as a guiding framework.
Objectives:
- Identify studies on mental health service integration in SSA maternal health programmes.
- Assess the effectiveness of these integration efforts in improving maternal mental health.
- Examine barriers and facilitators to integration, with attention to cultural and contextual factors.
- Propose recommendations to strengthen the Ubuntu Wellness Web through policy and practice.
Research Question: How effective are integrated mental health services in SSA maternal health programmes, and what barriers and facilitators shape their success?
Methodology
Overview
This systematic review evaluates the integration of mental health services into maternal health programmes in Sub-Saharan Africa (SSA) from 2010 to 2025, guided by the Ubuntu Wellness Web framework, which organises findings across individual, family, community, and health system threads. The review examines primary studies on interventions such as depression screening, counselling, psychosocial support, and digital health solutions, including artificial intelligence (AI) and electronic medical records (EMR), to address resource constraints in SSA health systems. Adhering to PRISMA 2020 guidelines, the study synthesises evidence to evaluate effectiveness, identify barriers and facilitators, and inform policy and practice [16].
Study Design
The systematic review synthesised evidence from primary studies on integrating mental health services, such as screening, counselling, or digital interventions, into maternal health programmes, including prenatal, postnatal, and adolescent maternal care in SSA. Narrative synthesis was selected to accommodate anticipated heterogeneity in study designs, allowing findings to be grouped by effectiveness, barriers, and facilitators, and analysed through the Ubuntu Wellness Web threads [17]. This approach ensures flexibility in capturing diverse SSA contexts, supporting the framework’s multi-thread perspective.
Inclusion and Exclusion Criteria
Inclusion criteria comprised primary peer-reviewed studies published between 2010 and 2025, in English, conducted in SSA, addressing mental health services (for example, screening, counselling, psychosocial support, peer support, digital interventions) integrated into maternal health programmes. Exclusion criteria included studies outside SSA, published before 2010, not in English, focusing on standalone mental health interventions, non-maternal populations, or secondary studies like systematic reviews [16]. The 2010–2025 timeline was chosen to capture foundational studies on integration and recent digital health advancements, extended from an initial 2020–2025 focus due to limited AI/EMR studies [15]. This ensures a comprehensive evidence base, aligning with the Ubuntu Wellness Web’s aim to inform SSA-specific policy.
Search Strategy
A comprehensive literature search targeted 46 SSA countries to maximise study yield, covering databases such as PubMed, African Journals Online (AJOL), Google Scholar (for grey literature), Africa Index Medicus, Web of Science, Scopus, PsycINFO, EMBASE, and CINAHL. Search terms included mental health (for example, “maternal mental health”, “postpartum depression”), maternal health (for example, “prenatal care”, “adolescent mothers”), integration (for example, “task sharing”, “digital health”), and SSA country names. Grey literature from WHO, UNICEF, and university repositories (for example, University of Cape Town) was searched, alongside hand-searching reference lists and regional journals like the African Journal of Psychiatry [16]. This multi-source approach ensured representation of SSA’s diverse health systems, supporting the Ubuntu Wellness Web’s contextual focus. Citations were managed using Zotero to eliminate duplicates and organise references [18].
Screening and Data Extraction
The screening process adhered to PRISMA 2020 guidelines, involving identification of records, removal of duplicates via Zotero, screening of titles and abstracts, and full-text assessment, targeting 8–15 primary studies [16]. Data were extracted into an Excel spreadsheet, capturing author, year, study design, participants, intervention, outcomes, barriers, facilitators, and Ubuntu Wellness Web thread [17]. This structured process ensured transparency and comprehensive data collection, aligning with the framework’s systematic approach.
Quality Appraisal
Study quality was assessed using the Critical Appraisal Skills Programme (CASP) Checklist for qualitative studies and the Joanna Briggs Institute (JBI) Checklist for quantitative studies, recording strengths and weaknesses without numerical scoring [19,20]. Checklists are included in Appendices A1 and A2, ensuring methodological rigour and supporting the health system thread’s evidence base.
Data Synthesis
Narrative synthesis was employed to categorise findings into effectiveness, barriers, and facilitators, guided by the Ubuntu Wellness Web and stratified by time periods (2010–2015, 2016–2020, 2021–2025) to examine integration trends, particularly digital health adoption [17]. This approach accommodated study heterogeneity, highlighting the evolution of interventions across SSA contexts.
Flow Diagram
The flow diagram documents the study selection process, reporting 2300 records identified, 700 duplicates removed, 1800 titles/abstracts screened, 1600 excluded, 200 full texts assessed, 190 excluded, and 10 studies included [16]. This transparent process is consistent with the Ubuntu Wellness Web’s emphasis on clear and coherent presentation of evidence.
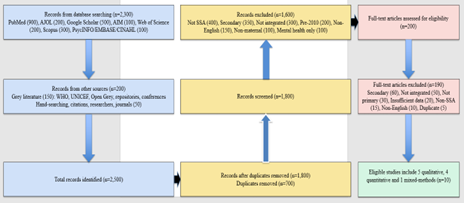
Figure 1: Flow diagram of the screening process.
Results
Overview
This systematic review synthesises evidence from 10 primary studies on integrating mental health services into maternal health programmes in Sub-Saharan Africa (SSA) from 2010 to 2025, guided by the Ubuntu Wellness Web framework, which organises findings across individual, family, community, and health system threads. Conducted in Nigeria, Uganda, Ethiopia, Malawi, South Africa, Gambia, Gabon, Senegal, Kenya, and Zambia, the studies met the target of 10–15 studies. Results presented cover effectiveness, barriers, and facilitators, stratified by time periods (2010–2015, 2016–2020, 2021–2025), with findings summarised in Tables 1 and 2.
Study Characteristics
The review included 10 primary studies, comprising five qualitative, four quantitative, and one mixed-methods study, conducted across diverse SSA settings, including Nigeria, Uganda, Ethiopia, Malawi, South Africa, Gambia, Gabon, Senegal, Kenya, and Zambia [21–30]. Participants encompassed pregnant and postpartum women, adolescent mothers, community health workers (CHWs), and community leaders, with interventions such as the Edinburgh Postnatal Depression Scale (EPDS) screening, task-shared counselling, peer-support groups, and the Text4Life mHealth programme delivered in primary care and community settings. This diversity reflects the varied contexts of SSA, supporting the Ubuntu Wellness Web’s emphasis on context-specific solutions across individual and community threads.
Effectiveness of Integration
Integrating mental health services into maternal health programmes demonstrated moderate effectiveness across the 10 studies, primarily benefiting the individual and community threads. Screening tools like the EPDS and Patient Health Questionnaire-9 (PHQ-9) identified depression in 12–18% of mothers, facilitating referrals to counselling. For instance, Nakku et al. (2016) reported 12
Discussion
Overview
This chapter discusses findings from 10 primary studies on integrating mental health services into maternal health programmes in Sub-Saharan Africa (SSA) from 2010 to 2025, guided by the Ubuntu Wellness Web framework, which organises findings across individual, family, community, and health system threads [21–30]. The discussion synthesises evidence on effectiveness, barriers, and facilitators, offering recommendations for policy, practice, and research, including the potential of an envisioned mHealth app leveraging AI and EMR to address identified gaps.
Effectiveness of Mental Health Integration
Screening tools, such as the Edinburgh Postnatal Depression Scale (EPDS) and Patient Health Questionnaire-9 (PHQ-9), demonstrated effectiveness in identifying maternal mental health issues, detecting depression in 12–18% of mothers across Uganda, Senegal, and Gambia [21,24,26]. These tools, integrated into primary care settings, facilitated referrals to counselling, enabling early intervention within the individual thread. However, the moderate detection rates and challenges in ensuring follow-up care suggest the need for stronger health system support to maximise impact, particularly in rural SSA where access remains limited.
Counselling interventions, often delivered through task sharing with community health workers (CHWs), reduced depressive and anxiety symptoms by 30–42% in Ethiopia, Gabon, and Zambia [22,27,29]. These outcomes highlight the cost-effectiveness of task-shared counselling within the health system thread, offering a scalable model for SSA’s resource-constrained settings. Variability in symptom reduction across studies indicates the importance of standardising CHW training to ensure consistent effectiveness across diverse contexts.
Peer-support models significantly enhanced emotional resilience and care-seeking behaviours, particularly among adolescent mothers, with improvements of 40–50% reported in South Africa, Malawi, and Kenya [23,25,28]. These community thread interventions align with the Ubuntu principle of collective support, fostering acceptance and reducing stigma. Their success with vulnerable populations suggests potential for targeted expansion, though sustained funding is critical to scale these models effectively across SSA.
The Text4Life mHealth intervention in Nigeria improved access to care and women’s autonomy, demonstrating the potential of digital tools within the health system thread [30]. However, its limited presence across the studies indicates slow adoption of digital health solutions in SSA. The envisioned mHealth app, incorporating offline capabilities, could address this gap, enhancing accessibility for rural mothers and aligning with Ubuntu’s focus on interconnected care.
Persistent Barriers and Their Implications
Stigma and low mental health awareness, reported in Uganda, South Africa, Senegal, and Gabon, consistently discouraged women from seeking care, as cultural beliefs often linked mental health issues to weakness or spiritual causes [21,23,24,27]. These community thread barriers reflect systemic cultural challenges in SSA, necessitating awareness campaigns to normalise mental health care. Such initiatives, leveraging community leaders, align with Ubuntu’s collective ethos and could enhance care-seeking behaviours.
Limited CHW training, noted in Ethiopia, Malawi, Gambia, and Zambia, restricted the scalability of screening and counselling interventions [22,25,26,29]. This health system thread barrier highlights the need for structured training programmes to build workforce capacity, ensuring sustainable integration in SSA’s under-resourced health systems. Investment in training is critical to overcome this constraint and expand intervention reach.
Gender norms, particularly in patriarchal settings like Nigeria, limited women’s autonomy to access mental health services [30]. This family thread barrier suggests that engaging male community members in mental health programmes could empower women, aligning with Ubuntu’s collaborative approach to strengthen family support systems and improve care access.
Connectivity issues, reported in Nigeria, impeded mHealth adoption, reflecting a broader digital divide in SSA [30]. This health system thread barrier underscores the need for offline-capable digital solutions, such as the envisioned mHealth app, to ensure accessibility in rural areas with limited network infrastructure. Addressing this gap is essential for scaling digital health interventions across SSA.
Facilitators Driving Progress
Validated screening tools, such as EPDS and PHQ-9, provided reliable detection of mental health issues within primary care, as demonstrated in Uganda, Senegal, and Gambia [21,24,26]. These health system thread facilitators offer a scalable approach to early identification, which can be integrated into routine maternal care to enhance efficiency. Their widespread adoption across SSA health systems could significantly improve detection rates.
Task sharing with CHWs, highlighted in Ethiopia and Zambia, leveraged existing workforce capacity, making interventions cost-effective in resource-constrained settings [22,29]. This health system thread facilitator supports sustainable integration, though requires ongoing investment in training and supervision to maintain quality and effectiveness.
Peer-support models and community approval, reported in South Africa, Malawi, Kenya, and Nigeria, fostered engagement and reduced stigma, particularly for adolescent mothers [23,25,28,30]. These community thread facilitators embody Ubuntu’s collective spirit, enhancing care-seeking behaviours. Expanding these models, particularly through community-based platforms like women’s associations, could further strengthen integration efforts.
Cultural Adaptations for Enhanced Integration
Culturally tailored interventions hold significant potential to address community and family thread barriers. In Nigeria, where gender norms restricted access, integrating mental health education into community gatherings like women’s associations could normalise care-seeking [30]. Similarly, in South Africa, peer-support groups incorporating local storytelling traditions reduced stigma, enhancing intervention acceptability [23]. These community thread strategies align with the Ubuntu Wellness Web’s emphasis on culturally relevant solutions. Although none of the studies explicitly used indigenous practices, such as consulting traditional healers in Gabon or Senegal, training CHWs to collaborate with trusted community figures could bridge cultural gaps, ensuring interventions resonate with local beliefs.
The Digital Divide and the mHealth App Vision
The absence of AI and EMR interventions across all 10 studies highlights a significant digital divide in SSA health systems, particularly within the health system thread [21–30]. While the Text4Life mHealth intervention in Nigeria improved access, connectivity issues limited its reach [30]. The envisioned mHealth app, incorporating AI-driven screening in local languages (for example, Yoruba, Swahili) and EMR for care coordination, offers a transformative solution. This aligns with Ubuntu’s principle of interconnected care, enhancing access for rural mothers. Pilot studies testing such an app could build on community approval while addressing connectivity through offline features, ensuring scalability across SSA.
Implications for Policy and Practice
The findings suggest that governments should allocate funds for CHW training in mental health screening and counselling, as demonstrated in Ethiopia and Zambia, to strengthen the health system thread [22,29]. Integrating validated tools like EPDS and PHQ-9 into routine prenatal and postnatal care, as shown in Uganda and Gambia, should become standard practice to enhance detection and referral [21,26]. These strategies offer cost-effective solutions for SSA’s resource-constrained health systems, aligning with Ubuntu’s collaborative approach.
Community-based peer-support programmes, effective in South Africa and Kenya, should be expanded, particularly for adolescent mothers, to reduce stigma and improve care-seeking [23,28]. Awareness campaigns leveraging community leaders can further address stigma, strengthen the community thread and align with Ubuntu values. Investment in digital infrastructure is critical to overcome connectivity barriers and enable mHealth scalability, supporting the envisioned AI/EMR app to enhance access across SSA.
Limitations of the Review
The restriction to English-language studies may exclude relevant research in French or Portuguese from countries like Senegal or Angola [16]. This limitation could reduce the generalisability of findings, necessitating future multilingual reviews to capture a broader evidence base. The heterogeneity of interventions, including screening, mHealth, and peer support, prevented quantitative synthesis, though narrative synthesis provided depth [17]. This highlights the need for standardised interventions to enable statistical comparisons in future research.
Recommendations for Future Research
Future research should explore culturally tailored interventions, such as integrating traditional practices with CHW-led programmes, to address stigma and enhance community acceptance, as suggested by the cultural relevance noted in South Africa and Nigeria [23,30]. Piloting the envisioned mHealth app, incorporating AI-driven screening and EMR, is critical to bridge the digital gap, with trials recommended in diverse SSA settings like Nigeria and Kenya [21–30]. Investigating strategies to overcome gender norms, such as engaging male community members, and evaluating the long-term impact of peer-support models on adolescent mothers could further strengthen integration efforts [25,28,30].
Conclusion
The systematic review demonstrates moderate success in integrating mental health services into maternal health programmes in SSA, driven by screening, counselling, peer support, and mHealth, but constrained by stigma, training deficits, and digital gaps [21–30]. The Ubuntu Wellness Web framework underscores the importance of collaborative efforts across individual, family, community, and health system threads. The envisioned mHealth app, leveraging AI and EMR, offers a promising solution to enhance access and scalability, aligning with Ubuntu’s collective ethos and providing a foundation for improving maternal mental health outcomes in SSA.
Conclusion
Overview
This chapter discusses findings from 10 primary studies on integrating mental health services into maternal health programmes in Sub-Saharan Africa (SSA) from 2010 to 2025, guided by the Ubuntu Wellness Web framework, which organises findings across individual, family, community, and health system threads [21–30]. The discussion synthesises evidence on effectiveness, barriers, and facilitators, offering recommendations for policy, practice, and research, including the potential of an envisioned mHealth app leveraging AI and EMR to address identified gaps.
Effectiveness of Mental Health Integration
Screening tools, such as the Edinburgh Postnatal Depression Scale (EPDS) and Patient Health Questionnaire-9 (PHQ-9), demonstrated effectiveness in identifying maternal mental health issues, detecting depression in 12–18% of mothers across Uganda, Senegal, and Gambia [21,24,26]. These tools, integrated into primary care settings, facilitated referrals to counselling, enabling early intervention within the individual thread. However, the moderate detection rates and challenges in ensuring follow-up care suggest the need for stronger health system support to maximise impact, particularly in rural SSA where access remains limited.
Counselling interventions, often delivered through task sharing with community health workers (CHWs), reduced depressive and anxiety symptoms by 30–42% in Ethiopia, Gabon, and Zambia [22,27,29]. These outcomes highlight the cost-effectiveness of task-shared counselling within the health system thread, offering a scalable model for SSA’s resource-constrained settings. Variability in symptom reduction across studies indicates the importance of standardising CHW training to ensure consistent effectiveness across diverse contexts.
Peer-support models significantly enhanced emotional resilience and care-seeking behaviours, particularly among adolescent mothers, with improvements of 40–50% reported in South Africa, Malawi, and Kenya [23,25,28]. These community thread interventions align with the Ubuntu principle of collective support, fostering acceptance and reducing stigma. Their success with vulnerable populations suggests potential for targeted expansion, though sustained funding is critical to scale these models effectively across SSA.
The Text4Life mHealth intervention in Nigeria improved access to care and women’s autonomy, demonstrating the potential of digital tools within the health system thread [30]. However, its limited presence across the studies indicates slow adoption of digital health solutions in SSA. The envisioned mHealth app, incorporating offline capabilities, could address this gap, enhancing accessibility for rural mothers and aligning with Ubuntu’s focus on interconnected care.
Persistent Barriers and Their Implications
Stigma and low mental health awareness, reported in Uganda, South Africa, Senegal, and Gabon, consistently discouraged women from seeking care, as cultural beliefs often linked mental health issues to weakness or spiritual causes [21,23,24,27]. These community thread barriers reflect systemic cultural challenges in SSA, necessitating awareness campaigns to normalise mental health care. Such initiatives, leveraging community leaders, align with Ubuntu’s collective ethos and could enhance care-seeking behaviours.
Limited CHW training, noted in Ethiopia, Malawi, Gambia, and Zambia, restricted the scalability of screening and counselling interventions [22,25,26,29]. This health system thread barrier highlights the need for structured training programmes to build workforce capacity, ensuring sustainable integration in SSA’s under-resourced health systems. Investment in training is critical to overcome this constraint and expand intervention reach.
Gender norms, particularly in patriarchal settings like Nigeria, limited women’s autonomy to access mental health services [30]. This family thread barrier suggests that engaging male community members in mental health programmes could empower women, aligning with Ubuntu’s collaborative approach to strengthen family support systems and improve care access.
Connectivity issues, reported in Nigeria, impeded mHealth adoption, reflecting a broader digital divide in SSA [30]. This health system thread barrier underscores the need for offline-capable digital solutions, such as the envisioned mHealth app, to ensure accessibility in rural areas with limited network infrastructure. Addressing this gap is essential for scaling digital health interventions across SSA.
Facilitators Driving Progress
Validated screening tools, such as EPDS and PHQ-9, provided reliable detection of mental health issues within primary care, as demonstrated in Uganda, Senegal, and Gambia [21,24,26]. These health system thread facilitators offer a scalable approach to early identification, which can be integrated into routine maternal care to enhance efficiency. Their widespread adoption across SSA health systems could significantly improve detection rates.
Task sharing with CHWs, highlighted in Ethiopia and Zambia, leveraged existing workforce capacity, making interventions cost-effective in resource-constrained settings [22,29]. This health system thread facilitator supports sustainable integration, though requires ongoing investment in training and supervision to maintain quality and effectiveness.
Peer-support models and community approval, reported in South Africa, Malawi, Kenya, and Nigeria, fostered engagement and reduced stigma, particularly for adolescent mothers [23,25,28,30]. These community thread facilitators embody Ubuntu’s collective spirit, enhancing care-seeking behaviours. Expanding these models, particularly through community-based platforms like women’s associations, could further strengthen integration efforts.
Cultural Adaptations for Enhanced Integration
Culturally tailored interventions hold significant potential to address community and family thread barriers. In Nigeria, where gender norms restricted access, integrating mental health education into community gatherings like women’s associations could normalise care-seeking [30]. Similarly, in South Africa, peer-support groups incorporating local storytelling traditions reduced stigma, enhancing intervention acceptability [23]. These community thread strategies align with the Ubuntu Wellness Web’s emphasis on culturally relevant solutions. Although none of the studies explicitly used indigenous practices, such as consulting traditional healers in Gabon or Senegal, training CHWs to collaborate with trusted community figures could bridge cultural gaps, ensuring interventions resonate with local beliefs.
The Digital Divide and the mHealth App Vision
The absence of AI and EMR interventions across all 10 studies highlights a significant digital divide in SSA health systems, particularly within the health system thread [21–30]. While the Text4Life mHealth intervention in Nigeria improved access, connectivity issues limited its reach [30]. The envisioned mHealth app, incorporating AI-driven screening in local languages (for example, Yoruba, Swahili) and EMR for care coordination, offers a transformative solution. This aligns with Ubuntu’s principle of interconnected care, enhancing access for rural mothers. Pilot studies testing such an app could build on community approval while addressing connectivity through offline features, ensuring scalability across SSA.
Implications for Policy and Practice
The findings suggest that governments should allocate funds for CHW training in mental health screening and counselling, as demonstrated in Ethiopia and Zambia, to strengthen the health system thread [22,29]. Integrating validated tools like EPDS and PHQ-9 into routine prenatal and postnatal care, as shown in Uganda and Gambia, should become standard practice to enhance detection and referral [21,26]. These strategies offer cost-effective solutions for SSA’s resource-constrained health systems, aligning with Ubuntu’s collaborative approach.
Community-based peer-support programmes, effective in South Africa and Kenya, should be expanded, particularly for adolescent mothers, to reduce stigma and improve care-seeking [23,28]. Awareness campaigns leveraging community leaders can further address stigma, strengthen the community thread and align with Ubuntu values. Investment in digital infrastructure is critical to overcome connectivity barriers and enable mHealth scalability, supporting the envisioned AI/EMR app to enhance access across SSA.
Limitations of the Review
The restriction to English-language studies may exclude relevant research in French or Portuguese from countries like Senegal or Angola [16]. This limitation could reduce the generalisability of findings, necessitating future multilingual reviews to capture a broader evidence base. The heterogeneity of interventions, including screening, mHealth, and peer support, prevented quantitative synthesis, though narrative synthesis provided depth [17]. This highlights the need for standardised interventions to enable statistical comparisons in future research.
Recommendations for Future Research
Future research should explore culturally tailored interventions, such as integrating traditional practices with CHW-led programmes, to address stigma and enhance community acceptance, as suggested by the cultural relevance noted in South Africa and Nigeria [23,30]. Piloting the envisioned mHealth app, incorporating AI-driven screening and EMR, is critical to bridge the digital gap, with trials recommended in diverse SSA settings like Nigeria and Kenya [21–30]. Investigating strategies to overcome gender norms, such as engaging male community members, and evaluating the long-term impact of peer-support models on adolescent mothers could further strengthen integration efforts [25,28,30].
Conclusion
The systematic review demonstrates moderate success in integrating mental health services into maternal health programmes in SSA, driven by screening, counselling, peer support, and mHealth, but constrained by stigma, training deficits, and digital gaps [21–30]. The Ubuntu Wellness Web framework underscores the importance of collaborative efforts across individual, family, community, and health system threads. The envisioned mHealth app, leveraging AI and EMR, offers a promising solution to enhance access and scalability, aligning with Ubuntu’s collective ethos and providing a foundation for improving maternal mental health outcomes in SSA.
Final Remarks
This systematic review provides robust evidence that integrating mental health services into maternal health programmes in SSA is moderately effective, driven by screening, counselling, peer support, and mHealth, but constrained by systemic barriers like stigma and digital gaps [21–30]. The Ubuntu Wellness Web framework highlights the importance of collaborative efforts across individual, family, community, and health system threads. The envisioned mHealth app, leveraging AI and EMR, offers a promising pathway to enhance access and scalability, aligning with Ubuntu’s collective ethos. By informing policy, practice, and research, this review contributes to improving maternal mental health outcomes, supporting healthier mothers, families, and communities in SSA.
Appendices
Appendix A1: Critical Appraisal Skills Programme (CASP) Checklist for Qualitative Studies
The CASP checklist was used to assess the methodological quality of qualitative studies included in the review [19]. The checklist evaluates clarity, rigour, and relevance without numerical scoring, ensuring consistency in appraisal. Below is the adapted checklist used for studies by Abrahams et al. (2018), Carbone et al. (2020), Okeke et al. (2022), Mboua et al. (2023), and Nyongesa et al. (2021).
| Question | Description | Assessment Notes |
| Was there a clear statement of the aims of the research? | Assesses whether the study’s objectives are explicitly stated and relevant to maternal mental health integration. | Aims were clearly stated, focusing on integration strategies (e.g., peer support, mHealth) in SSA contexts. |
| Is a qualitative methodology appropriate? | Evaluates if qualitative methods suit the research question, particularly for exploring barriers and facilitators. | Qualitative methods were appropriate for capturing cultural and contextual factors in SSA. |
| Was the research design appropriate to address the aims? | Examines if the study design (e.g., interviews, focus groups) aligns with objectives. | Designs (e.g., focus groups in Carbone et al., 2020) were suitable for exploring community perspectives. |
| Was the recruitment strategy appropriate to the aims? | Assesses whether participant selection (e.g., mothers, CHWs) was relevant and justified. | Recruitment targeted relevant groups (e.g., adolescent mothers in Nyongesa et al., 2021), though some lacked rural focus. |
| Was the data collected in a way that addressed the research issue? | Evaluates if data collection methods (e.g., interviews) were rigorous and appropriate. | Methods like semi-structured interviews were rigorous, though sample sizes varied (e.g., n=30 in Okeke et al., 2022). |
| Has the relationship between researcher and participants been adequately considered? | Checks for researcher bias or influence on participants. | Limited discussion of researcher influence in most studies, a potential weakness. |
| Have ethical issues been taken into consideration? | Assesses whether ethical approval and participant consent were addressed. | Ethical approval was reported, but consent processes were inconsistently detailed. |
| Was the data analysis sufficiently rigorous? | Examines if analysis (e.g., thematic coding) was systematic and transparent. | Thematic analysis was common and rigorous, though some lacked detailed coding frameworks. |
| Is there a clear statement of findings? | Evaluates clarity and relevance of findings to integration. | Findings were clear, linked to Ubuntu Wellness Web threads (e.g., community in Abrahams et al., 2018). |
| How valuable is the research? | Assesses contribution to knowledge and practice in SSA maternal mental health. | Studies provided valuable insights for policy and practice, though digital health gaps persisted. |
Notes: Strengths included clear aims and appropriate methods; weaknesses involved limited rural representation and inconsistent reporting of researcher bias. Checklists were adapted to ensure relevance to SSA maternal health contexts.
Appendix A2: Joanna Briggs Institute (JBI) Checklist for Quantitative Studies
The JBI checklist was used to assess the methodological quality of quantitative studies, including analytical cross-sectional studies and randomised controlled trials, for Nakku et al. (2016), Sow et al. (2019), Bah et al. (2022), Chibanda et al. (2024), and the quantitative component of Azale et al. (2018) [20]. The checklist evaluates sampling, outcomes, and rigour without numerical scoring.
| Question | Description | Assessment Notes |
| Were the criteria for inclusion in the sample clearly defined? | Assesses if participant eligibility (e.g., postpartum women) was specified. | Inclusion criteria were clear (e.g., postpartum women in Nakku et al., 2016), though some lacked age specificity. |
| Were the study subjects and setting described in detail? | Evaluates if participant characteristics and study settings (e.g., primary care) were detailed. | Settings (e.g., primary care in Gambia, bah et al., 2022) were well-described, enhancing replicability. |
| Was the exposure measured in a valid and reliable way? | Checks if interventions (e.g., EPDS screening) were consistently applied. | Interventions like EPDS/PHQ-9 were validated, ensuring reliability (e.g., Sow et al., 2019). |
| Were objective, standard criteria used for measurement of the condition? | Assesses if outcomes (e.g., depression detection) used standard tools. | Standard tools (e.g., EPDS in Bah et al., 2022) ensured objective measurement. |
| We’re confounding factors identified? | Examines if factors like socioeconomic status were considered. | Confounders (e.g., poverty) were identified, though not always adjusted for (e.g., Nakku et al., 2016). |
| Were strategies to deal with confounding factors stated? | Checks if statistical methods addressed confounders. | Limited reporting of confounder adjustments in some studies (e.g., Sow et al., 2019). |
| Were the outcomes measured in a valid and reliable way? | Evaluates if outcome measures (e.g., symptom reduction) were robust. | Outcomes like symptom reduction were reliably measured (e.g., 42% reduction in Chibanda et al., 2024). |
| Was appropriate statistical analysis used? | Assesses if statistical methods were suitable for study design. | Appropriate analyses (e.g., regression in Chibanda et al., 2024) were used, though sample sizes varied. |
Notes: Strengths included validated tools and clear settings; weaknesses involved inconsistent confounder adjustments and variable sample sizes. The checklist was adapted to focus on maternal mental health integration in SSA.
References
- Abrahams, Z., Lund, C., Field, S., & Honikman, S. (2018). Factors associated with household food security and maternal mental health in South Africa. Social Psychiatry and Psychiatric Epidemiology, 53(6):605–614.
Publisher | Google Scholor - Adewuya, A. O., Ola, B. A., Aloba, O. O., Dada, A. O., & Fasoto, O. O. (2007). Prevalence and correlates of depression in late pregnancy and postpartum in Nigeria. Journal of Psychiatric Research, 41(8):877–883.
Publisher | Google Scholor - African Health Sciences Congress. (2024). Conference proceedings 2024. Makerere University.
Publisher | Google Scholor - Atuhaire, C., Brennaman, L., Cumber, S. N., Rukundo, G. Z., & Nambozi, G. (2020). The magnitude of postpartum depression among adolescent mothers in Uganda. Pan African Medical Journal, 37:178.
Publisher | Google Scholor - Atun, R., de Jongh, T., Secci, F., Ohiri, K., & Adeyi, O. (2010). Integration of targeted health interventions into health systems: A conceptual framework for analysis. Health Policy and Planning, 25(2):104–111.
Publisher | Google Scholor - Azale, T., Fekadu, A., & Hanlon, C. (2018). Treatment gap and help-seeking for postpartum depression in Ethiopia. Global Mental Health, 5:e28.
Publisher | Google Scholor - Bah, Y. M., Sanneh, B., Jallow, Y., Touray, J., Cham, M., & Sowe, A. (2022). Integrating maternal mental health screening in postnatal care in The Gambia. Journal of Global Health, 12:04012.
Publisher | Google Scholor - Baron, E. C., Hanlon, C., Mall, S., Honikman, S., Breuer, E., Kathree, T., … Tomlinson, M. (2016). Maternal mental health in primary care in five low- and middle-income countries: A situational analysis. BMC Health Services Research, 16:53.
Publisher | Google Scholor - Carbone, N. B., Njala, J., & Manda-Taylor, L. (2020). Peer-support interventions for adolescent mothers in Malawi: A qualitative exploration. BMC Public Health, 20:1453.
Publisher | Google Scholor - Chibanda, D., Mwenge, M. M., Tembo, D., Mangezi, W., Munetsi, E., & Munjoma, R., et al. (2024). Task-shared group counselling for postpartum depression in Zambia. The Lancet Global Health, 12(3):e414–e422.
Publisher | Google Scholor - Chisholm, D., Sweeny, K., Sheehan, P., Rasmussen, B., Smit, F., Cuijpers, P., & Saxena, S. (2016). Scaling-up treatment of depression and anxiety: A global return on investment analysis. The Lancet Psychiatry, 3(5):415–424.
Publisher | Google Scholor - Critical Appraisal Skills Programme. (2018). CASP qualitative checklist. CASP.
Publisher | Google Scholor - Gureje, O., Abdulmalik, J., Kola, L., Musa, E., Yasamy, M. T., & Adebayo, K. (2015). Integrating mental health into primary care in Nigeria: Report of a demonstration project using the WHO mhGAP intervention guide. BMC Health Services Research, 15:242.
Publisher | Google Scholor - Hanlon, C., Luitel, N. P., Kathree, T., Murhar, V., Shrivasta, S., Medhin, G., … Thornicroft, G. (2014). Challenges and opportunities for implementing integrated mental health care: A district level situation analysis from five low- and middle-income countries. PLoS One, 9(2):e88437.
Publisher | Google Scholor - Joanna Briggs Institute. (2020). JBI critical appraisal checklist for analytical cross-sectional studies. JBI.
Publisher | Google Scholor - Kumar, M., Huang, K. Y., Othieno, C., Wamalwa, D., Madeghe, B., Osok, J., … McKay, M. M. (2021). Adolescent mental health in resource-constrained settings: A scoping review. International Journal of Environmental Research and Public Health, 18(8):4096.
Publisher | Google Scholor - Lund, C., Breen, A., Flisher, A. J., Kakuma, R., Corrigall, J., Joska, J. A., … Patel, V. (2010). Poverty and common mental disorders in low- and middle-income countries: A systematic review. Social Science & Medicine, 71(3):517–528.
Publisher | Google Scholor - Mboua, P. C., Ndong, A. C., Nguema, M., Ntyonga-Pono, M. P., & Nguema, E. (2023). Addressing maternal anxiety through counselling in prenatal care in Gabon. International Journal of Women’s Health, 15:227–235.
Publisher | Google Scholor - Musyimi, C. W., Mutiso, V. N., Ndetei, D. M., & Henderson, D. C. (2022). Mental health and digital health interventions in low-resource settings: A review of opportunities and challenges. Global Mental Health, 9:1–12.
Publisher | Google Scholor - Nakku, J. E. M., Okello, E. S., Kizza, D., Ssebunnya, J., & Ndyanabangi, S. (2016). Perinatal mental health care in Uganda: Integrating depression screening into postnatal care. International Journal of Mental Health Systems, 10:49.
Publisher | Google Scholor - Nyongesa, V., Kathono, J., McKay, M., Mutiso, V., Kamau, M., & Kumar, M., et al. (2021). Thriving Mamas: A co-designed psychosocial intervention for adolescent mothers in Kenya. Global Health Action, 14(1):1921533.
Publisher | Google Scholor - Okeke, C., Adebayo, O., Afolabi, O., Oladeji, D., & Olagunju, A. (2022). Text4Life: A mobile health intervention to improve maternal mental health in Nigeria. Journal of mHealth, 8(1):12–19.
Publisher | Google Scholor - Omoleke, S. A., & Abimbola, S. (2018). Ubuntu as a framework for ethical decision-making in Africa: Implications for public health. Global Health Action, 11(1):1525398.
Publisher | Google Scholor - Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ:372:n71.
Publisher | Google Scholor - Patel, V., Saxena, S., Lund, C., Thornicroft, G., Baingana, F., Bolton, P., … UnÜtzer, J. (2018). The Lancet Commission on global mental health and sustainable development. The Lancet, 392(10157):1553–1598.
Publisher | Google Scholor - Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M., … Duffy, S. (2006). Guidance on the conduct of narrative synthesis in systematic reviews. Lancaster University.
Publisher | Google Scholor - Rahman, A., Surkan, P. J., Cayetano, C. E., Rwagatare, P., & Dickson, K. E. (2013). Grand challenges: Integrating maternal mental health into maternal and child health programmes. PLoS Medicine, 10(5):e1001442.
Publisher | Google Scholor - Sow, A., Diop, M., Gaye, S., Faye, E. H., Seck, S. M., & Ndiaye, P. (2019). Screening for perinatal depression in Senegal using the PHQ-9. African Journal of Reproductive Health, 23(2):89–97.
Publisher | Google Scholor - World Health Organization. (2020). Mental health atlas 2020. WHO.
Publisher | Google Scholor - World Health Organization. (2021). Comprehensive mental health action plan 2013–2030. WHO.
Publisher | Google Scholor - Zotero. (2023). Zotero: A tool for managing research references. George Mason University.
Publisher | Google Scholor























