

Research Article
In-Depth Investigation of The Adult Measles Epidemic in The Meiganga Health District, Adamawa Region-Cameroon, 2023
- Djamilatou Leila 1,3
- Antsele Onanena Blondel 1,4*
- Mohamad Anouar Al- Sadat 2
- Asakizi Nji Augustine 4
1Adamawa Public Heath Delegation, MoH, Cameroon.
2Meiganga Heath District, Adamawa Region-MoH, Cameroon.
3Faculty of Medicine and Biomedical Sciences, University of Garoua, Cameroon.
4School of Health and Medical Sciences, Kesmond International University, Cameroon.
*Corresponding Author: Antsele Onanena Blondel, School of Health and Medical Sciences, Kesmond International University, Cameroon
Citation: Leila D., Blondel A.O., Al-Sadat M.A., Augustine A.N. (2025). In-Depth Investigation of The Adult Measles Epidemic in The Meiganga Health District, Adamawa Region-Cameroon, 2023, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 4(1):1-10. DOI: 10.59657/2997-6103.brs.25.077
Copyright: © 2025 Antsele Onanena Blondel, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 04, 2025 | Accepted: June 30, 2025 | Published: July 04, 2025
Abstract
Measles, an infant airborne disease is a significant public health issue in Adamawa region, with 08/11 Heath Districts (HD) affected in 2023. Meiganga HD recorded a measles outbreak and the aim of the investigation was to describe cases in time-place-person, find additional cases, conduct a Rapid Vaccine Coverage Survey (RVCS) and evaluate the measles surveillance system. A cross- sectional study was conducted in August 2023. Line-listing was used to describe cases in time- place-person. Active case-finding was done using case definition from the Guide for Integrated Disease Surveillance and Response. The Simplify Lot Quality Assurance Sampling method and a questionnaire were used for the RVCS. The 2001 CDC guidelines was used to evaluate measles surveillance system. For quantitative data, medians, means and proportions were calculated using MS_Excel and Epinfo. QGis3.6 software helped for spatial representation. In total, 19 cases were recorded with 15(68.2%) male (M/F sex-ratio 2:1). The median age was 20[0.5-52] years and 18(81.8%) cases were over five years old. All cases presented with a maculopapular rash and fever, along with 15(68.2%) also had cough and 12(54,5%) had conjunctivitis. Only 3(13.6%) cases were vaccinated, 3(13.6%) had zero-dose and 16(72.7%) had unknown vaccination status. The first case occurred in Epi_Week_2 but the peak was in Epi_Week_28 despite the Measles-Rubeola (MR) response campaign in Epi_Week_27. Babongo were the most affected health area with 12(54.5%) cases. Active case finding helped to discovery 3(13.2%) additional cases. For RVCS, 78 children aged 9-59 months were surveyed, of whom 75(97.4%) received one dose of MR1 vaccine, 22(28.5%) received the MR2 dose and 3(3.8%) were zero-dose. The measles surveillance system was useful, simple and acceptable. The completeness and timeliness were moderately acceptable. We administered the zero-dose vaccine and raised community awareness of importance of vaccination. The measles outbreak occurred among adults despite the MR campaign. We recommended the respect of vaccination schedule.
Keywords: measles; outbreak; investigation; vaccination
Introduction
According to the World Health Organization (WHO, 2021), public health surveillance is the systematic and continuous collection of relevant data, its effective consolidation and evaluation, and the rapid dissemination of results to those concerned, particularly those in a position to take action. Measles is a highly contagious viral infection and one of the diseases under surveillance in Cameroon. Measles deaths increased by 50% worldwide between 2016 and 2019 (WHO, 2019). Measles is a public health problem in the Adamawa region in view of the three recent epidemics recorded this year, with 111 suspected cases (DHIS2, 2021). Measles is a highly contagious viral infection. The virus is transmitted either directly through contact with the nasopharyngeal secretions of infected individuals, or indirectly through persistence of the virus in the air or on a surface contaminated by nasopharyngeal secretions (CDC, 2009). After an incubation period of 8 to 12 days (Signore, 2001), fever (around 38.3°C) and malaise appear within 24 hours (Ray, 2004). The onset of the rash varies from 7 to 23 days, but averages 14 days (WHO,2018). These symptoms are followed by cough, coryza (inflammation of the nasal mucosa) and conjunctivitis. After 2 to 3 days of coughing, coryza and conjunctivitis, Koplik spots (white, granular lesions on the lateral oral mucosa) appear. On the fourth day, a macropapular rash appears on the face and neck. The rash then spreads to the rest of the body, persisting for 3 to 5 days before fading (Signore, 2001). Anorexia and dyspnea are other symptoms of measles (Shimatsu & Fujimori, 1999). Serious complications are more common before the age of 5 and in adults over 30. Among the most serious complications are blindness, encephalitis (which can be accompanied by cerebral edema), severe diarrhea, ear infections and severe respiratory infections such as pneumonia (WHO, 2019). The leading cause of death is pneumonia in children and acute encephalitis in adults. Measles outbreaks can lead to epidemics with the potential to cause large numbers of deaths. The vast majority of measles deaths (over 95%) occur in countries with low per capita incomes and weak health infrastructures. Measles deaths increased by 50% worldwide between 2016 and 2019 (WHO, 2019). Diagnosis must be confirmed biologically, and is based on the detection of measles virus-specific IgM in serum. Samples must be taken between days 3th and 28th after the onset of the rash, ensuring that there has been no recent vaccination.
According to the Guide for Integrated Disease Surveillance and Response in Cameroon (IDSR Guide, 2020), the alert threshold is crossed if five suspected cases are reported over four consecutive weeks in a health district, and the epidemic threshold is crossed if three laboratory-confirmed cases are reported over four consecutive epidemiological weeks in a Health District (HD). Active case finding consists of identifying people who have presented signs compatible with measles (fever, maculopapular rash, cough, coryza or conjunctivitis) and have had contact with a confirmed case or have been exposed in the same spatio-temporal setting (WHO, 2017). WHO (2018) aims to eliminate this disease through high vaccination coverage and enhanced surveillance. In Epidemiological Week (EW) 33_2023, five suspected cases of measles were notified by the Babongo Integrated Health Center (IHC) in the Meiganga HD, Adamawa-Cameroon region, despite the widespread Measles-Rubella (MR) vaccination campaign in EW 17 of the same year. The aim of the investigation was to describe cases in Time-Place-Person (TPP), find additional cases, conduct a Rapid Vaccine Coverage Survey (RVCS) and evaluate the measles surveillance system.
Materials and Methods
Type, Location and Study Period
A descriptive cross-sectional study was carried out in the Meiganga HD, Adamawa region, in August 2023. This health district comprises 18 Health Areas and 26 health facilities, 20 of which are public and 6 privates.
Study Population
The source population consisted of all people living in the Meiganga HD during the study period.
Selection Criteria
Inclusion Criteria:
- Cases Description in TPP: Any person presenting with signs and symptoms of measles in the Meiganga HD during the study period;
- Active Case-Finding: All persons meeting the definition of a suspected case of measles in the DS of Meiganga in the last four weeks;
- RVCS: All the persons aged 9-59 months in the Meiganga HD during the study period;
- Evaluation of the Measles Surveillance System: All players in measles surveillance at the district health service and in the health facilities of the Meiganga HD.
Exclusion Criteria: Any person meeting the above-mentioned inclusion criteria, but refusing to participate in the study or absent at the time of the survey.
Sampling
Sampling Techniques
Cases Description in TPP: An exhaustive sampling of all cases and deaths found in the Meiganga HD was used.
Active Case-Finding: Two-stage stratified sampling was used:
- Stage 1: In the community, an exhaustive sampling of people living in communities in health areas that had notified at least one case of measles was used.
- Stage 2: In health facilities, an exhaustive sample of health facilities in health areas that had reported at least one case of measles in the last four weeks was used.
RCVS: Three-stage stratified sampling was used:
- Stage 1: Choice of health areas, an exhaustive sample of health areas in Meiganga HD having notified at least one case of measles in the last four weeks was used.
- Stage 2: Selection of villages, a random sample of three villages per health area having notified at least one case of measles in the last four weeks was used.
- Stage 3: Choice of households, cluster sampling was used. All consecutive households in the cluster with children aged 9-59 months were included in the study, for a total of 10 children per village.
Evaluation of the Measles Surveillance System: we used a stratified three-stage sampling:
- Stage 1: Selection of health areas, an exhaustive sample of health areas in Meiganga HD having notified at least one case of measles in the last four weeks was used.
- Stage 2: Selection of health facilities, an exhaustive sample of health facilities in health areas that had reported at least one case of measles in the last four weeks was used.
- Stage 3: selection of respondents: respondents were randomly selected from the health department of the Health Department and the departments of the health facilities, with three staff per facility.
Sample Size
Table 1: Sample size by specific objective for investigation of measles epidemic, Meiganga HD.
| Specific Objectives | Source Population | Sample Size |
| Cases Description in TPP | All Suspected/Confirmed Cases | / |
| Active Case-Finding | Community | / |
| Health Training | 3 Health Facilities | |
| RCVS | Health Areas | 3 Health Areas |
| Villages | 9 Villages | |
| People | 90 Children 0-59 Months | |
| Evaluation of the Monitoring System | Health Area | 3 Health Areas |
| Health Training | 3 Health Facilities | |
| Healthcare Workers | 16 Health Personnel |
Data Collection
Collection Tools
Cases Description in TPP: The line listing of measles cases has enabled us to describe cases in TPP.
Active Case-Finding: We used the case definition adapted from the IDSR Technical Guide for Cameroon.2020), contextualized to the Meiganga HD.
Suspect Case: Any person, resident in the Meiganga HD, presenting with fever, generalized maculo-papular rash with cough or rhinorrhea or conjunctivitis, or any person in whom the doctor suspects measles.
Community Case Definition: Any person living in the Meiganga HD who presented with fever, generalized maculo-papular rash and/or cough and/or a cold and/or conjunctivitis (red eyes) or any person in whom the clinician suspected measles in a period dating back 30 days (07/17/2023) prior to the time of the survey.
Confirmed Case: Suspected case (or any person) in whom the laboratory found positive measles-specific IgM serology and/or any person meeting the definition of suspected case and having an epidemiological link with the outbreak.
RCVS: A pre-tested questionnaire was used, including observations (respondents' vaccination card).
Evaluation of the Measles Surveillance System: A pre-tested and validated questionnaire and observation form were used to collect data.
Collection Procedure
Cases Description in TPP: We used the line listing of measles cases available from the Meiganga HD and questioned suspected cases found during the active case finding.
Active Case-Finding: We carried out an active case finding to identify additional cases in health facilities and in the community:
- In the health facilities, we carried out a review of the consultation registers of the reception and emergency services in the health facilities having notified at least one case of measles during the last 4 weeks, in the DS.
- In the community, we looked for additional cases around the cases in the communities to capture any cases missed during the last four weeks.
RCVS: We used a classification system based on the "Simplify Lot Quality Assurance Sampling" method. This system classifies coverage on a three-step scale (low if coverage is below 50%, medium if between 50% and 85%, and high if above 85%).
Evaluation of the Measles Surveillance System: The aim was to describe the organization of the measles surveillance system, the resources allocated to it, their roles in the system and attribute measurement. Attributes were evaluated according to the CDC guidelines of Robert German's working group (Robert Germann, 2001). We assessed three qualitative attributes (usefulness, simplicity and acceptability) and two quantitative attributes (completeness and timeliness).
Usefulness
Was considered to be the ability of the surveillance system to use the data collected by the system for public health decisions/actions in the Meiganga HD. In other words, the role of the data collected by the system in decision-making. The system was said to be useful for a score of 80%-100%, moderately useful for a score of 79%-50% and not useful if less than 50%.
Simplicity
Was the fact of having an efficient, easy-to-use structure, clear and precise case definition, rapid and standardized measles data collection and transmission procedures, in the Meiganga HD. The system was said to be simple for a score of 80% to 100%, moderately simple for a score of 79% to 50% and not simple for a score of less than 50%.
Acceptability
Was the willingness and commitment of staff involved in surveillance to participate in the measles surveillance and response process in Meiganga HD. The system was deemed acceptable for a score of 80% to 100%, moderately acceptable for a score of 79% to 50% and not acceptable for a score of less than 50%.
Completeness
Was considered to be the system's ability to identify and report all cases of measles in Meiganga HD and ensure that those involved in surveillance complete all surveillance tools (forms, registers, linear lists, etc.), as well as all variables contained in these tools. Completeness was judged to be good for a proportion ≥90%, average for a proportion 50-79% and poor for a proportion below 50%.
Timeliness
Was considered to be the system's ability to notify all cases of measles and take appropriate action without delay between any two or more steps in the Meiganga HD. Timeliness was considered good for a proportion ≥80%, average for a proportion between 50-79% and poor for a proportion below 50%.
Data Processing and Analysis
Microsoft Excel 2016 spreadsheet software was used to generate tables, graphs and curves, as well as to determine the various rates, ratios and proportions for qualitative variables, and measures of central tendency (means, mode, median...) for quantitative variables. QGIS 3.18.3 software was used to produce a spatial representation of the cases.
Ethical Considerations and Data Confidentiality
All activities were carried out in strict compliance with administrative procedures, involving stakeholders at different levels, notably regional, district, health facility and community. After obtaining informed consent, interviews were conducted in a confidential and anonymous setting. The data were secured on a password-protected computer.
Results
Description of TPP Cases
Time: The graph below shows the evolution of measles cases and deaths in the Meiganga HD.
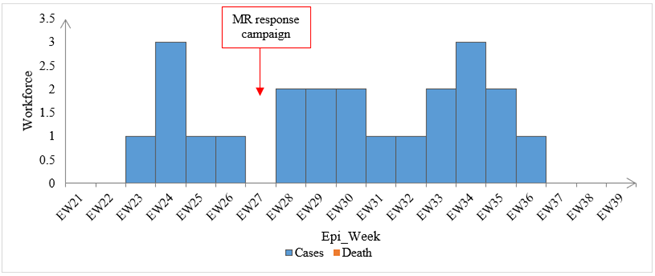
Figure 1: Number of measles cases and deaths in the Meiganga HD, Adamawa Region, 2023.
The number of cases fluctuated, reflecting the spread of the epidemic, with two peaks of 3 cases each at EW_24 and EW_34, despite the measles-rubella vaccination campaign at EW_27.
Place: The map below shows the spatial distribution of measles cases in the Meiganga HD.
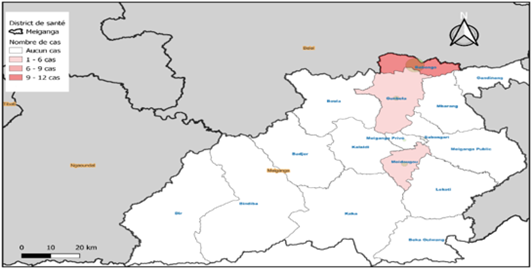
Figure 2: Spatial distribution of measles cases in Meiganga HD, Adamawa Region, 2023.
The Babongo health area was the most affected with 12(54.5%) cases, followed by the neighboring Gumbéla health area with 6(27.3%) cases and the Meidougou health area with 4(18.2%) cases.
Person
Age and Gender: The distribution of measles cases by age and sex is shown in the figure below:
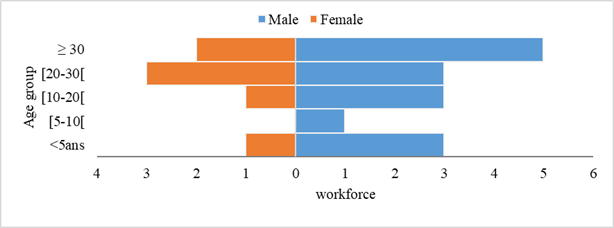
Figure 3: Distribution of cases by age and sex in Meiganga HD, Adamawa Region, 2023.
Men were the most affected, with 15(68.2%) cases, representing a 2:1 M/F sex ratio. The median age was 20[0.5-52] years and 18(81.8%) cases were over five years old.
Signs and Symptoms: The distribution of measles cases according to signs/symptoms is shown in the figure below:
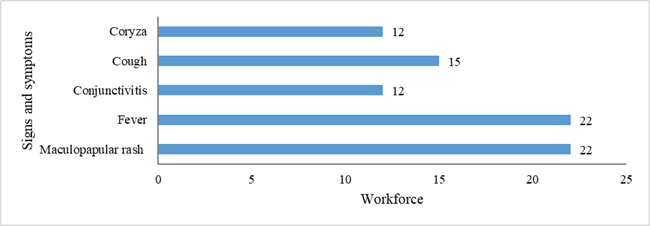
Figure 4: Distribution of cases by signs/symptoms in Meiganga HD, Adamawa Region, 2023.
All cases presented with fever and maculopapular rash. Cough was present in 15 (68.2%) cases and conjunctivitis in 12 (54.5%).
Vaccination Status: The figure below shows the distribution of measles cases according to vaccination status:
Figure 5:Distribution of cases by signs/symptoms in Meiganga HD, Adamawa Region, 2023.
This revealed that 16(72.7%) cases had unknown vaccination status and 3(13.63%) cases were unvaccinated.
Clinical Management
A total of 9 (40.9%) cases reported having been hospitalized for an average of around two days at the Babongo IHC. The treatment administered to these hospitalized cases was mainly: Penicillin G: 1miilion/8h; Ringer Lactate: 500cc/12h; Paracetamol injection and Vitamin A.
Case Fate
Of the 22 cases recorded, 20 (90.9%) recovered their health and 2 (9.1%) were still active and under treatment.
Active Case-Finding
In Health Facilities: The active search for additional cases in the health facilities consisted in reviewing the consultation registers and was based on the case definition. This led to the identification of 3 (13.6%) additional cases, which were added to the linear list.
In The Community: The active search for additional cases in the community was based on the notions of contact and measles case definition. Of the 22 cases recorded, 9 (40.9%) declared having been in contact with a sick person, and the circumstances of contact were most often within the family. Following this community search, no additional active cases were found.
Rapid Vaccine Coverage Survey
A total of 78 children belonging to the vaccination target of the routine Expanded Program on Immunization (9-59 months) were surveyed, of whom 45 (57.7%) were male, i.e., a 1:1 M/F sex ratio. The median age was 36 [9-59] months, and the most represented age group was [24-59] months, i.e., 61 (78.2%) children. The table below shows the results of the RR vaccine rapid coverage survey.
Table 2: MR vaccine coverage during vaccinations, Meiganga HD, August 2023.
| Vaccination Appointment | Number (%) | Classification of Vaccine Coverage | ||
| Vaccinated | Unvaccinated | Total | ||
| MR1 | 75(97,4%) | 3(3,6%) | 78(100%) | High |
| MR2 | 22(28,5%) | 56(71,5%) | 78(100%) | Low |
| MR Campaign | 72(93,6%) | 6(4,4%) | 78(100%) | High |
Of the 78 children surveyed, 76 (97.4%) had received at least one dose of RR vaccine at all three appointments. Overall, 75 (97.4%) children had received a dose of RR1 vaccine and only 22 (28.5%) had received a dose of RR2 vaccine. During the RR follow-up and response campaign in July 2023, 72(93.6%) children were vaccinated. This enabled us to classify the different MR vaccine coverages in these localities.
Evaluation of the Measles Surveillance System
Description of the measles Surveillance System
In the Meiganga HD, the measles surveillance system is in line with the national strategy for surveillance of measles and other vaccine-preventable diseases. The system is based on an early warning mechanism through community surveillance by Community Health Workers (CHWs). After notification by the CHWs, the alert is then validated by the health facility's surveillance focal point and the DS management team, who carry out a preliminary investigation accompanied by blood sampling. Nevertheless, the vast majority of cases are detected passively in health facilities during consultations. The case definition used is that of the IDSR Technical Guide, adapted from that of the WHO. After sampling, samples are forwarded to the Regional Biological Sample Reception Station (RBSRS) against reimbursement of transport costs. In turn, the Regional RBSRS forwards the samples to the National RBSRS, housed at the Groupe Technique Central du Programme Elargie de Vaccination (GTC PEV), via a local transport agency. The National RBSRS forwards the samples to the CPC for analysis and case confirmation. Test results are communicated to the regional level, which in turn forwards them to the district health service. The alert threshold is crossed if five suspected cases are reported in the DS over a period of four consecutive weeks, and the epidemic threshold is crossed if three cases are confirmed by the laboratory in the DS over a period of four consecutive weeks. This early detection of cases enables better clinical management and infection control. The Meiganga HD has a surveillance protocol containing defined objectives, case definitions, data transmission circuits, data analysis and validation procedures, but no data protection procedures. The epidemic monitoring and management committee exists, but does not meet regularly. Nevertheless, a few meetings have been mentioned by the district management team, but are not documented (attendance lists and reports). The epidemic management committee provided feedback to the health facilities and communities concerned.
Measuring Measles Surveillance System Attributes
The summary of the evaluation of the attributes of the measles surveillance system in the Meiganga HD is shown in the table below:
Table 3: Summary of measles surveillance system attributes in Meiganga HD, 2023.
| Measles Surveillance System Attributes | Average Score for Health Facilities | District Health Service Score | Evaluator Score | Total Score | System Qualification |
| Usefulness | 92% | 100% | 100% | 90% | Useful |
| Simplicity | 97% | 100% | 100% | 99% | Simple |
| Acceptability | 75% | 100% | 67% | 80% | Acceptable |
| Completeness | 80% | 67% | 67% | 71% | Average |
| Timeliness | 81% | 67% | 67% | 71% | Average |
The measles surveillance system was useful, simple and acceptable. The completeness and timeliness were moderately acceptable.
Public Health Measures
- Making IDSR Technical Guides available to health facilities with shortages;
- Notification circuit available for display in health facilities;
- Search for missed cases of other diseases in consultation registers;
Raising community awareness of the importance of vaccination for disease prevention, and above all of the need to adhere to the vaccination schedule.
Discussion
Cases Description in TPP
Men were the most affected, with 15(68.2%) cases. The median age was 20[0.5-52] years and 18(81.8%) cases were over five years old. No deaths were recorded. A total of 16(72.7%) cases had unknown vaccination status and 3(13.6%) cases were unvaccinated. Cases continued to be recorded after the RR response campaign, i.e., 16(72.7%) cases. These results contradict those of Ketema Belda et al (2017), who reported a case-fatality rate of 0.2% in an investigation of a measles epidemic in Ethiopia, with the majority of cases (77.5%) aged under 15 and 48% aged under 5. In the same study, 70% of cases had not received any vaccine, and cases gradually declined after the response campaign. Factors such as promiscuity, movement of people in the affected health areas and poor vaccine storage conditions during the MR campaign could explain the resurgence of cases despite the RR campaign. This assertion is corroborated by the results of a study on factors associated with the occurrence of measles epidemics in Cameroon (Esum Mathias et al., 2023). Our results also differ from those of Marcellin Mengouo Nimpa et al. (2020) in a study carried out in Madagascar in which the median age of measles cases was 7 years, with the majority of cases (50.6%) aged under 9 years and a case-fatality rate of 1.2%. The unvaccinated status of children, their history of contact with measles cases, their travel history, and the presence of cases in the family or among neighbors are factors associated with high prevalence and recurrent measles infections (Daniel Eshetu et al., 2024).
Active Case-Finding
Active search for additional cases revealed 3(13.6%) cases in health facilities and no cases in the community, despite the fact that 9(40.9%) cases reported having been in contact with a sick subject, and the circumstances of contact were most often within the family. CHWs were involved, as studies have shown that the use of community workers and local health structures improves case detection (Goodson JL et al., 2011). Our results differ from those of a study conducted in Nigeria, which found that active search tripled the number of cases identified compared with passive notification (Fagbami AH & Dosumu-Ogunbi, 2018). Constraints such as late mobilization of investigation teams, inadequate staff training and lack of logistics (transport, fuel) may have limited the effectiveness of active search for additional cases (Grais RF et al., 2007).
Rapid Vaccine Coverage Survey
RVCS results were acceptable for MR1 appointments and the MR follow-up and response campaign, but poor for MR2. Our results are similar to those of Fausta Michael et al (2024), who reported vaccine coverage of 90% for MR1 and poorer performance for MR2. Furthermore, the emerging incident cases in adults may not be directly linked to recent vaccinations, but to past vaccinations, given that only 4(18.2%) cases belong to the age group concerned by routine vaccination and the target of the RR response campaign. This suggests that other factors, such as poor vaccination coverage in the past or the presence of unvaccinated Central African refugees, could be at the origin of this epidemic. These results are in line with those of Ryoko Sato et al (2022) in a study in Nigeria on the correlation between the incidence of measles epidemics and RR vaccination coverage. Also, the decline in routine vaccination coverage between the years 2020 and 2022, due to the COVID-19 pandemic, could have influenced the emergence of this outbreak. This corroborates the results of a study carried out in Croatia by Drenjancevic (2022) and those of a study carried out in Ghana by Michael Rockson Adjei (2024) on the impact of immunization coverage on the epidemiology of measles-rubella, which highlighted the importance of setting up effective protocols to ensure complete immunization, even during health crises. Thus, interventions including effective coordination, free case management, reactive vaccination, strengthening real-time surveillance, communication and community engagement, and revitalization of routine immunization should be adopted (Vincent Dossou et al., 2020 & Mukhlid Yousif et al., 2022).
Evaluation of the Measles Surveillance System
Usefulness: The system was deemed "useful" because it enables cases to be identified so that appropriate preventive measures can be rapidly put in place (reinforcement of routine vaccination in target areas). It can detect changes in trends or epidemic episodes through monitoring and analysis of alert and action thresholds. The system provides reliable quantified estimates of measles-related morbidity and mortality (1 case per 10,000 inhabitants). The system identifies risk factors for the onset and spread of the disease, based on the vaccination status of cases, their mapping, and the search for additional cases among contacts. The system thus helps to improve disease prevention and control. The data produced by the system can be used to generate hypotheses on the extent and prediction of the evolution of the situation, the sex (sex ratio M/F 2:1) and age groups most affected (over 5 years old), and high-risk areas (Babongo Health Area with 12 cases). All this enables us to target an efficient and appropriate response according to priorities. The system makes it possible to pool resources and strengthen early detection and coordinated response to outbreaks (Perry HN et al. 2007). Nevertheless, deficits are observed in the biological confirmation of all cases, which can have an impact on data quality. This situation is similar to that in several African countries (Masresha BG et al., 2021). However, challenges remain, particularly in terms of staff training, supervision and the use of data for decision-making (Nsubuga P, et al., 2002).
Simplicity: The system was described as "simple" because the data flow and task descriptions are straightforward and understood by everyone involved in the system. Use of the case definition is simple and understood by all. Use of the notification form is simple, as it can be completed in less than 5 minutes. The procedure for sending data is simple and understood by all those involved in the system. However, the weak point of the system's simplicity is the multiplicity of forms used to declare a case (consultation register, notification form, investigation form), as well as the multiplicity of reporting tools (linear list, DHIS2, RMA). In addition, case confirmation is carried out at several levels and by several actors. Our results are similar to those of Mara F. et al, (2022) in a study on the evaluation of the measles surveillance system in the HD of Kérouané in Guinea, where the system was judged to be simple.
Acceptability: The system is deemed "acceptable" because all personnel involved in the measles surveillance system are effectively involved in surveillance (register review, investigation, notification) and response where appropriate. The response report is drafted and forwarded to the regional and central authorities. The weak point linked to the acceptability of the system remains the absence of weekly surveillance meetings, with archiving of the reports of said meetings. Our results corroborate those of Mara F. et al, (2022) in a study on evaluating the measles surveillance system in the HD of Kérouané in Guinea, where the system was deemed acceptable.
Completeness: The completeness of the measles surveillance system in Meiganga HD was rated as "average", as the MS_Excel spreadsheet is used for reporting and data analysis. All cases were reported in DHIS2. An evaluation of the measles surveillance system in Miamey health district (Habibatou et al., 2021) presented similar results. All cases are included in the linear list, but not all the variables in the list are well filled in. For each case, the various forms (notification and investigation) are filled in and properly arranged. Nevertheless, not all variables are correctly filled in, especially for suspected cases with negative laboratory results. The same applies to variables entered in consultation registers. Laboratory data are not available for all cases. Efforts must be made to strengthen regional laboratory networks, but lack of technical and logistical capacity remains a major obstacle in several countries (Rota PA & Moss WJ., 2020).
Timeliness: The timeliness of the measles surveillance system was rated as "average", as it enabled early detection of cases. The time between detection of suspected cases and notification is always respected (immediately). The time between the start of the rash and sampling is respected (between day 3thand day 28th). The time between sampling and forwarding of samples to the national RBSRS is always respected (less than 72 hours), thanks to financial support from WHO. The time between receipt of results and transmission to the lower level is also respected (immediately). However, the ideal time between detection of the index case and the end of the search for additional cases (3 days) has not been respected. This contradicts WHO standards on the time taken to search for missed cases (WHO, 2017).
Conclusion
At the end of our investigation, we found a total of 22 cases in consultation registers and in the community. Measles is a childhood disease, but the vast majority of cases were adults over the age of 20. No deaths were recorded. The vaccination status of almost all cases was unknown (memory bias), but routine vaccination coverage and that of the previous campaign were satisfactory for children aged between 9 and 59 months, with the exception of the second dose of RR2 vaccine. The active search for missed cases was an essential component of the investigation. It enables a better estimate of the spread of the virus, a targeted and rapid response, and a reduction in morbidity. However, its effectiveness depends on the quality of team preparation, community involvement and speed of intervention. Nevertheless, only three additional cases were found in health facilities, and no additional cases were found in the community. Regular and rigorous evaluation of the measles surveillance system is essential if we are to make progress towards its elimination. Despite the progress made, gaps remain in many contexts, requiring targeted corrective action, strong political commitment and sustained investment. This has led us to reinforce staff and community awareness of measles case definition, management and hygiene measures, and the importance of consuming vitamin A-rich foods. The line listing of suspected measles cases in the district has also been updated. We recommend continuing surveillance for measles and other vaccine-preventable diseases, intensifying public awareness of hygiene and vaccination, holding weekly surveillance meetings, reinforcing routine EPI through advanced strategies, and providing constant feedback to lower-level authorities.
References
- Atkinson, W. (2006). Epidemiology and Prevention of Vaccine-Preventable Diseases. Department of Health & Human Services, Centers for Disease Control and Prevention.
Publisher | Google Scholor - Eshetu, D., Tosisa, W., Regassa, B. T., Hundie, G. B., Mulu, A. (2024). Epidemiology of Measles Outbreaks, Incidence and Associated Risk Factors in Ethiopia from 2000 to 2023: A Systematic Review and Meta-Analysis. BMC Infectious Diseases, 24(1):914.
Publisher | Google Scholor - Drenjančević, I., Samardžić, S., Stupin, A., Borocz, K., Nemeth, P., et al. (2022). Measles Vaccination and Outbreaks in Croatia from 2001 to 2019; A Comparative Study to Other European Countries. International Journal of Environmental Research and Public Health, 19(7):4140.
Publisher | Google Scholor - Eyong, E. M., Njoh, A. A., Etutu, S. J. M., Bachir, H. B., Ndoula, S. T., et al. (2023). Factors Associated with Measles Outbreak in Three Health Districts of Cameroon In 2019: A Cross-Sectional Study. Pan African Medical Journal, 46(1).
Publisher | Google Scholor - Fagbami AH, Dosumu-Ogunbi O. (2018). Active Search for Measles Cases During Outbreaks: A Key Component of Effective Surveillance. Bull World Health Organ. 96(3):225-230.
Publisher | Google Scholor - Michael, F., Mirambo, M. M., Misinzo, G., Minzi, O., Beyanga, M., et al. (2024). Trends of Measles in Tanzania: A 5-Year Review of Case-Based Surveillance Data, 2018-2022. International Journal of Infectious Diseases, 139:176-182.
Publisher | Google Scholor - German, R. R., Horan, J. M., Lee, L. M., Milstein, B., Pertowski, C. A. (2001). Updated Guidelines for Evaluating Public Health Surveillance Systems; Recommendations from the Guidelines Working Group. Recommendations and Reports: Morbidity and Mortality Weekly Report. 50(13):25-30.
Publisher | Google Scholor - Goodson, J. L., Masresha, B. G., Wannemuehler, K., Uzicanin, A., Cochi, S. (2011). Changing Epidemiology of Measles in Africa. The Journal of Infectious Diseases, 204(suppl_1):S205-S214.
Publisher | Google Scholor - Grais, R. F., Dubray, C., Gerstl, S., Guthmann, J. P., Djibo, A., et al. (2007). Unacceptably High Mortality Related to Measles Epidemics in Niger, Nigeria, and Chad. PLoS Medicine, 4(1):e16.
Publisher | Google Scholor - Habibatou, I. D. E., Yanogo, P. K., Djibo, I., Togola, O. B., Diallo, F., et al. (2021). Evaluation of the Measles Epidemiological Surveillance System in Niamey Health District II from 2017 to 2019. Sciences de la Santé, 44(2):62-71.
Publisher | Google Scholor - Belda, K., Tegegne, A. A., Mersha, A. M., Bayenessagne, M. G., Hussein, I., et al. (2017). Measles Outbreak Investigation in Guji Zone of Oromia Region, Ethiopia. The Pan African Medical Journal, 27(Suppl 2):9.
Publisher | Google Scholor - Herida, M. (2016). Methods for Evaluating Public Health Surveillance Systems.
Publisher | Google Scholor - Mara, F., Ngona, M. C., Corvil, S. (2022). Evaluation of the measles surveillance system - Kérouané health district, Guinea August 2020. Revue d'Épidémiologie et de Santé Publique, 70:S214.
Publisher | Google Scholor - Nimpa, M. M., Andrianirinarison, J. C., Sodjinou, V. D., Douba, A., Masembe, Y. V., et al. (2020). Measles outbreak in 2018-2019, Madagascar: Epidemiology and Public Health Implications. Pan African Medical Journal, 35(1).
Publisher | Google Scholor - Masresha BG, Hatcher C, Lebo E, Tanifum P, Bwaka AM, et al. (2023). Progress Toward Measles Elimination - African Region, 2017-2021. MMWR Morb Mortal Wkly Rep. 72(36):985-991.
Publisher | Google Scholor - Adjei, M. R., Longsignikuu, A., Iddris, I. S., Suuri, T. N., Asamoah, B., et al. (2024). Trend of Measles-Rubella Vaccination Coverage and Impact on Measles Epidemiology in the Savannah Region, Ghana; 2018-2022: A secondary data analysis. Vaccine, 42(8):1910-1917.
Publisher | Google Scholor - Cameroon Ministry of Public Health (2020). Technical Guide for Integrated Disease Surveillance and Response in Cameroon. Ed 2021:455-457.
Publisher | Google Scholor - Yousif, M., Hong, H., Malfeld, S., Smit, S., Makhathini, L., et al. (2022). Measles incidence in South Africa: a six-year review, 2015-2020. BMC Public Health, 22(1):1647.
Publisher | Google Scholor - Nsubuga, P., Eseko, N., Tadesse, W., Ndayimirije, N., Stella, C., et al. (2002). Structure and Performance of Infectious Disease Surveillance and Response, United Republic of Tanzania, 1998. Bulletin of the World Health Organization, 80:196-203.
Publisher | Google Scholor - Perry, H. N., McDonnell, S. M., Alemu, W., Nsubuga, P., Chungong, S., et al. (2007). Planning an Integrated Disease Surveillance and Response System: a Matrix of Skills and Activities. BMC Medicine, 5:1-8.
Publisher | Google Scholor - Ray, C. G. (2004). Mumps virus, Measles, Rubella, and other Childhood Exanthems, Sherris. Medical Microbiology, 4th Edition, 513-539.
Publisher | Google Scholor - Rota PA, Moss WJ. (2020). Measles Surveillance and Laboratory Testing. J Infect Dis. 222(Suppl 5):S588-S593.
Publisher | Google Scholor - Sato, R., Makinde, O. A., Daam, K. C., Lawal, B. (2022). Geographical and Time Trends of Measles Incidence and Measles Vaccination Coverage and Their Correlation IN Nigeria. Human Vaccines & Immunotherapeutics, 18(6):2114697.
Publisher | Google Scholor - Shimatsu, Y., Fujimori, K. (1999). Pulmonary Complications in Adult Measles. Kansenshogaku Zasshi: The Journal of the Japanese Association for Infectious Diseases, 73(7):640-645.
Publisher | Google Scholor - Signore, C. (2001). Rubella. Primary Care Update for Ob/Gyns, 8(4):133-137.
Publisher | Google Scholor - Unicef. (2018). Coverage Survey of the Programme de Prise en Charge Intégrée de la Malnutrition Aigue Sévère (PCIMAS).
Publisher | Google Scholor - Sodjinou, V. D., Douba, A., Nimpa, M. M., Masembe, Y. V., Randria, M., et al. (2020). Madagascar 2018-2019 Measles Outbreak Response: Main Strategic Areas. Pan African Medical Journal, 37(1).
Publisher | Google Scholor - World Health Organization. (2017). Measles Surveillance: Guidelines for Case Investigation and Outbreak Response. Geneva: WHO.
Publisher | Google Scholor - World Health Organization. (2018). Surveillance Standards for Vaccine-Preventable Diseases. 2nd ed. Geneva: WHO.
Publisher | Google Scholor - World Health Organization (2019). News Room Fact Sheets Details Measles.
Publisher | Google Scholor - World Health Organization. (2021). Health Surveillance.
Publisher | Google Scholor























