

Case Report
Hyperparathyroidism Clinically Mimicking Multiple Myeloma: A Case Report
1Senior Resident, Department of Haematology, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi, India.
2Senior Consultant and Head, Department of Haematology, Sir Ganga Rama Hospital, Rajinder Nagar, New Delhi, India.
3Senior Consultant and Vice chairperson, Department of Haematology, Sir Ganga Rama Hospital, Rajinder Nagar, New Delhi, India.
4Associate Consultant, Department of Haematology, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi, India.
*Corresponding Author: Deepak Goel, Senior Resident, Department of Haematology, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi, India.
Citation: Goel D, Kotwal J, Langer S, Prakhar P. (2025). Hyperparathyroidism Clinically Mimicking Multiple Myeloma: A Case Report, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 4(5):1-3. DOI: 10.59657/2997-6103.brs.25.094
Copyright: © 2025 Deepak Goel, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 16, 2025 | Accepted: October 30, 2025 | Published: November 05, 2025
Abstract
Brown tumor is rare manifestation associated with hyperparathyroidism that may simulate metastatic bone disease or multiple myeloma and pose difficulty in differential diagnosis. Here, we report a case which was clinically suspected as multiple myeloma on basis of anemia, hypercalcemia and multiple lytic bone lesions but classical bone marrow features of osteotitis fibrosa cystic led to suspicion of hyperparathyroidism and helped to reach the final diagnosis. Hence, hypercalcemia and lytic bone lesions on imaging are not always due to malignant pathology but metabolic bone disease should also be considered in differential diagnosis.
Keywords: hypercalcemia; lytic bone lesions; hyperparathyroidm; multiple myeloma
Introduction
Two most common differential in patients with lytic bone lesion are metastatic bone tumor and multiple myeloma. Brown tumor is a rare benign condition (2 percent cases in patients with hyperparathyroidism) which may simulate malignancy and pose difficulty in differential diagnosis [1]. We describe a case of Primary hyperparathyroidism clinically mimicking multiple myeloma.
Case Presentation
A case of 36-year-old female who was referred from orthopedics department of clinical hematology with complaint of back pain, anemia (8.2 gm/dl), hypercalcemia (11.1 mg/dl) and multiple lytic lesions in pelvic and sacral bone on X-ray (Figure 1). Renal function test and liver function test were normal except markedly elevated serum alkaline phosphatase (593 U/L). Bone marrow was done to rule out multiple myeloma.

Figure 1: Digital X ray showing multiple lytic lesions in Ileum, pubic rami and right femur bone.
Bone marrow aspirate showed prominence of osteoblasts which is not normal findings at this age with 3% plasma cells. All other hemopoietic elements were in normal range. Bone marrow biopsy showed a hypocellular marrow with narrowing of marrow spaces with fibrosis and new cement lining with mineralization of trabeculae (osteosclerosis). Also, these areas show excess osteoid rimming around the bony trabeculae (like osteomalacia) (Figure 2,). Rest areas show normal cellularity with thinned out trabeculae with paratrabecular fibrosis and increased osteoclastic activity (Figure 3). Focal areas show cyst formation, hemosiderin laden macrophages and metastatic calcification. Reticulin Stain: Grade 2-3 fibrosis. So, features of bone marrow were consistent with osteotitis fibrosa cystica secondary to hyperparathyroidism due to any cause.
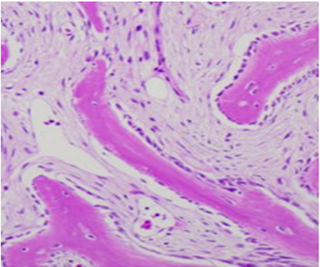
Figure 2: Osteoblastic rimming around bony trabeculae. (H&E x 1000).
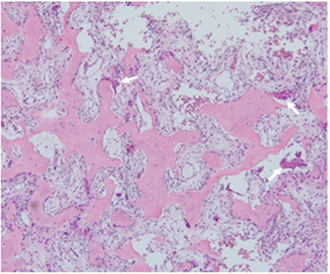
Figure 3: Microscopic examination of the right iliac bone biopsy showing high number of osteoclasts (arrows) (H&E x 100).
In view of this bone marrow features patients was called to hematology lab and extensively valued. Patient gave history of loose motion for 2 years, weight loss and severe bone pains. Her investigation reports showed normal renal function test with paradox of high serum calcium levels but low vitamin D3. Hence, parathyroid hormone level was advised which came out to be 1046 pg/ml (Normal range: 10-65 pg/mL). Patient was then referred to endocrinologist. USG neck was done which showed 5 x 12.9 mm hypodense lobulated space occupying lesion along inferior pole of right lobe of thyroid. Tc99m labeled parathyroid scan showed hyperfunctioning parathyroid tissue-adenoma. Surgical excision of the parathyroid adenoma was done. It was reported as parathyroid adenoma on histopathology. After normalization of serum parathyroid hormone level, the bony lesion resolved. The patient is now symptom free.
Discussion
Primary HPT (PHPT) is an endocrinopathic condition characterized by hypesecretion of parathyroid hormone (PTH), which may be caused by an adenoma (solitary or multiple), idiopathic hyperplasia, or a parathyroid carcinoma. Secondary HPT is characterized by hypocalcemia or Vitamin D deficiency acting as a stimulus of excessive PTH production. Chronic renal failure is the main cause of secondary HPT. Tertiary HPT is caused by the development of autonomous parathyroid hyperplasia after long - standing secondary HPT, most often in patients with renal failure. Most cases of PHPT (80% - 85%) are caused by a solitary adenoma, 15% to 20% are due to a parathyroid gland hyperplasia, and less than 0.5% are caused by parathyroid carcinoma [2,3]. Primary bone lesion (brown tumor). Skeltal involvement in hyperparathyroidism occur due to high rate of osteoclastic bone resorption and is accompanied by a cellular repair process that results in the accumulation of fibrous stroma and connective tissue cells along with multinucleated giant cells and occur more frequent in the carcinomas or secondary hyperparathyroidism than PHP [4,5]. Multiple lytic bone lesion is seen in all three condition- hyperparathyroidism, metastatic bone tumor and multiple myeloma (MM). But PHP more commonly involve cortical bones and bones distal to elbow, knee joint and facial skeletal (particularly mandible) while metastatic bone tumor and MM more commonly involve cancellous bone i.e., axial skeletal [5,6]. Hypercalcemia can occur in all three conditions. In our case multiple lytic bone lesion with hypercalcemia led to clinical suspicion of multiple myeloma but classical bone marrow biopsy features of hyperparathyroidism led to diagnosis of Primary hyperparathyroidism.
Conclusion
Our case report highlights the significance of high degree of suspicion and awareness that is required for reaching right diagnosis in a case presenting lytic bone lesion along with hypercalcemia. Lytic bone lesions together on imaging together with hypercalcemia are not always due to malignant pathology but metabolic bone disease should also be considered in differential diagnosis.
Declarations
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
References
- Ullah, E., Ahmad, M., Ali, S. A., Redhu, N. (2012). Primary hyperparathyroidism having multiple Brown tumors mimicking malignancy. Indian Journal of Endocrinology and Metabolism, 16(6):1040-1042.
Publisher | Google Scholor - Khan, A., Samtani, S., Varma, V. M., Frost, A., Cohen, J. (1994). Preoperative parathyroid localization: prospective evaluation of technetium 99m sestamibi. Otolaryngology-Head and Neck Surgery, 111(4):467-472.
Publisher | Google Scholor - Owens, B. B. (2009). A review of primary hyperparathyroidism. Journal of Infusion Nursing, 32(2):87-92.
Publisher | Google Scholor - Doshi, S., Vadi, A., Mahajan, A., Nagpal, T. (2012). Primary hyperparathyroidism with rare presentation as multiple brown tumours. Clinics and Practice, 2(2):e48.
Publisher | Google Scholor - Huang, R., Zhuang, R., Liu, Y., Li, T., Huang, J. (2015). Unusual presentation of primary hyperparathyroidism: report of three cases. BMC Medical Imaging, 15(1):23.
Publisher | Google Scholor - Su, A. W., Chen, C. F., Huang, C. K., Chen, P. C. H., Chen, W. M., et al. (2010). Primary hyperparathyroidism with brown tumor mimicking metastatic bone malignancy. Journal of the Chinese Medical Association, 73(3):177-180.
Publisher | Google Scholor























