

Research Article
Hialuxina: A Paradigm Shift in The Application of Botulinum Toxin/Hyaluronic Acid (TBTA)/(AH)
1Icron Medical Instituto, Santiago de Chile, Chile.
2Centro Latinoamericano de Entrenamiento Medico e Investigación CLEMI, Bogotá, Colombia.
*Corresponding Author: Gladys Velazco, Centro Latinoamericano de Entrenamiento Medico e Investigación CLEMI, Bogotá, Colombia.
Citation: Salerno I, Velazco G, Sequera M. (2026). Hialuxina: A Paradigm Shift in The Application of Botulinum Toxin/Hyaluronic Acid (TBTA)/(AH), International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 6(6):1-5. DOI: 10.59657/2997-6103.brs.26.138
Copyright: © 2026 Gladys Velazco, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 13, 2026 | Accepted: March 30, 2026 | Published: April 03, 2026
Abstract
Background: The combination of botulinum toxin type A (BTTA) and hyaluronic acid (HA) has been established as a synergistic and safe strategy for facial rejuvenation, improving dynamic and static wrinkles, skin texture, and prolonging treatment effects compared with monotherapy.
Objectives: To evaluate whether the combination of BTTA and HA improves wrinkles and cutaneous aging in a specific facial area to a greater extent and for a longer duration than BTTA alone or baseline conditions, and to assess safety, patient satisfaction, required doses/volumes, and duration of the effect.
Materials and Methods: A prospective study was conducted in 30 patients with moderate cutaneous aging who received a single combined session of BTX A and HA in the target area, and were assessed for efficacy, safety, and subjective satisfaction.
Results: Most patients showed clinical improvement in at least one of the evaluated variables, with predominant changes in the mandibular contour (jowls), followed by the periocular region and overall skin quality; 10 patients exhibited marked improvement in the jowls.
Conclusion: Combined BTTA and HA in a single session appears to be an effective and safe option with particular impact on the lower facial third, an area typically more resistant to minimally invasive treatments, consistent with previously reported studies.
Keywords: botulinum toxin; hyaluronic acid; aging; hyaluxin; subdermal
Introduction
The combination of botulinum toxin type A (BTTA) and hyaluronic acid (HA) has been established as a synergistic and safe strategy for the treatment of facial aging, improving dynamic and static wrinkles, skin texture, and the overall duration of results compared with monotherapy [1,2]. The physiopathological basis and rationale for this combination are that BTTA blocks acetylcholine release, reduces muscle hyperactivity and the mechanical traction on the skin, and is therefore more effective for dynamic wrinkles of the upper third of the face (forehead, glabella, periocular area) [3]. HA (cross-linked and non-cross-linked) restores volume, improves dermal hydration and elasticity, and is the treatment of choice for static wrinkles and gravitational folds [4]. The combination allows better control of dynamic wrinkles and greater dermal/subdermal structural support, providing a more comprehensive effect on the aging cascade (muscle-dermis-volume) and reducing the required BTTA dose and HA volume [5]. Studies with BTTA plus high-molecular-weight non-cross-linked HA compounds have shown significant improvement in pores, texture, and skin quality parameters at 1-4 months, with maintenance of the effect versus baseline [6]. We therefore propose a pilot study based on a controlled clinical trial to test the safety, feasibility, and signal of efficacy of the HA/BTTA combination. High-molecular-weight non-cross-linked HA has hygroscopic and viscoelastic properties that enhance skin hydration and restore barrier function [7]. The priority in this combination is the synergy of both compounds, which produces a dual biological effect: hydration and dermal reorganization mediated by water binding and the indirect stimulation of fibroblasts induced by HA, together with regulatory dermal neuromodulation that balances sebaceous and sweat gland function, reduces micro-contraction of superficial dermal fibers, and creates a favorable environment for tissue repair [5-7]. This interaction promotes controlled dermal mechanotransduction, optimizing the activity of fibroblasts, myofibroblasts, and endothelial cells, with an increase in type I and III collagen and improvement in cutaneous microcirculation [8,9]. Unlike cross-linked HA formulations, the mixture with non-cross-linked HA allows more homogeneous diffusion within the dermal plane, enhancing the bifunctional action without generating volume. The objective of this study was evaluated whether the combination of BTTA and HA improves wrinkles and cutaneous aging in a specific facial area to a greater extent and for a longer duration than BTTA alone or baseline conditions, and to assess safety, patient satisfaction, required doses/volumes, and duration of the effect.
Materials and Methods
The primary objective of this study was to evaluate whether the combination of BTTA and HA improves wrinkles/cutaneous aging in a specific area to a greater extent (and for a longer duration) than BTTA alone or baseline conditions; secondary objectives included safety, patient satisfaction, required doses/volumes, and duration of the effect. The efficacy and safety of the combination of BTX‑A and HA administered in a single session were assessed in patients with moderate skin aging (Glogau II-III). A parallel controlled trial using BTTA plus HA was conducted, designing specific injection points in the different facial thirds and evaluating subjects photographically (rater‑blinded) using standardized photographs.
Target Population: 30 women aged 45-70 years with impaired “skin quality”.
Inclusion Criteria: no prior aesthetic treatments in the area within the previous 6-12 months (BTTA, HA, laser, radiofrequency) and rhytidosis classified as Glogau II-III.
Exclusion Criteria: pregnancy/breastfeeding, neuromuscular diseases, allergy to any component, coagulation disorders, active infections, and unrealistic expectations.
Pilot Sample Size: 30 patients.
For the procedures, an injection design based on anthropometric points and specific measurements was proposed to allow reproducibility of the technique, referred to as the “dose map” (Figure 1).
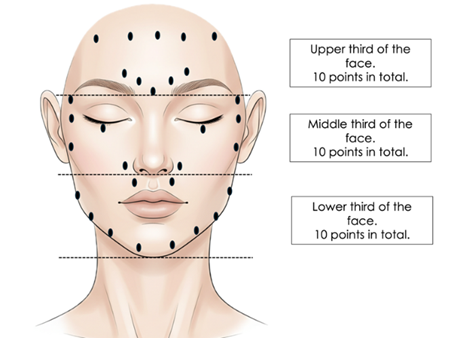
Figure 1: Dose map by facial third, indicating the areas to be treated in each third. Own source.
Subsequently, the mixture is prepared for administration by reconstituting one vial of onabotulinumtoxinA containing 100 biological units with 2 mL of normal saline solution (0.9% NaCl), since a higher dilution provides a larger volume that favors binding with hyaluronic acid. From this stock solution, 0.6 mL are withdrawn, equivalent to approximately 30 biological units of toxin. In parallel, a 2-mL vial of high-molecular-weight non-cross-linked hyaluronic acid is used; for this study, Hyaluromax Skin Builder L was employed, an ultrapure hyaluronic acid preparation containing 64 mg/2 mL, combining two hyaluronics: 32 mg of 1,800-kDa HA + 32 mg of L-HA of 2,500 kDa (Laboratorio Futerman, Argentina). Both components are carefully mixed in a sterile Luer-Lock syringe using aseptic technique, obtaining a homogeneous and slightly viscous solution. The resulting proportion is 30 U of botulinum toxin / 2 mL of non-cross-linked HA, a ratio that constitutes the standard to ensure a balance between biostimulation and peripheral neurological safety. It is worth noting that this mixture must be used immediately, without subsequent storage, due to the potential protein degradation of the toxin in hyaluronic media. Preparation is carried out under strict aseptic conditions and in a controlled environment (no exposure to light or high temperature). For the application, depending on the areas with greater rhytidosis, when only one facial third was treated, 0.2 mL per point were injected until completing ten points in each third, in a strictly subdermal injection plane (Figure 2).
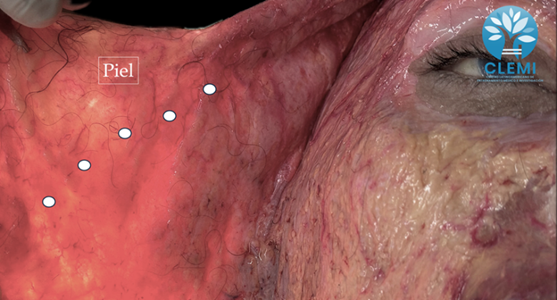
Figure 2: Superficial facial dissection showing separation of the dermal plane from the fat plane, indicating the specific locations of the Hialuxina injection points. Dissection performed at the Latin American Center for Medical Training and Research (CLEMI), Bogotá, Colombia. November 2025.
Results
The graph shows that, in a cohort of 30 patients, most experienced some degree of clinical improvement in at least one of the variables analyzed, with changes predominating in the mandibular contour (jowls), followed by the periocular region and overall skin quality. Ten patients showed improvement in the jowls, suggesting that the intervention has a particularly relevant impact on the lower facial third, an area that is usually more resistant to change with minimally invasive treatments, in line with reported studies [10]. Eight patients showed improvement in the periocular region, while six demonstrated improvement in skin texture or quality, indicating beneficial effects also in the midface and in global cutaneous parameters [11], although to a lesser extent than in the mandibular contour, which is expected given that neither the volumes nor the doses were high. Six patients did not show clinically relevant changes, which could be related to individual variability (age, phototype, aging pattern, comorbidities) or to differences in the technique and therapeutic plan applied (Figure 3).
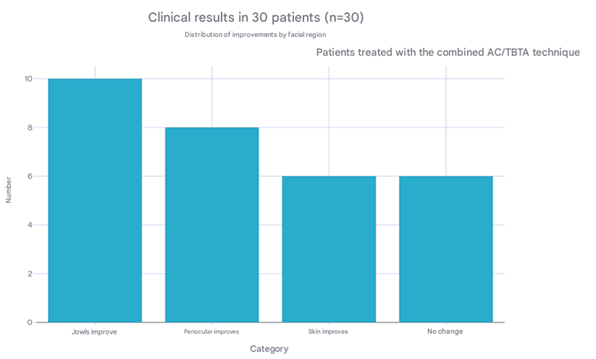
Figure 3: Graph: Clinical outcomes of 30 treated patients (n = 30) who underwent the Hialuxina technique.
Clinical trials and meta‑analyses have shown that HA fillers achieve clinically significant and long‑lasting corrections (up to 12-24 months) in malar volume and midface contour, with high responder rates on GAIS and MFVLR scales [12].
In the midface, relevant changes were observed, consisting of elevation of the malar complex, attenuation of nasolabial folds, and improvement in cheek contour and projection; however, in this study we did not use cross-linked hyaluronic acid, so it is suggested that these changes are related to improved accommodation of the structures, in line with what has been described for intradermal toxin and hyaluronic acid fillers in this region [10]. The changes demonstrated in this study are consistent with previously reported studies, with the caveat that this combination appears more stable and is associated with fewer complications.
In Figure 4, the changes observed at the malar and supraorbital levels can be seen, together with a reduction in the jowls (Figure 4).

Figure 4: Female patient, 46 years old. A: Before treatment, specific points marked with the dotted arrow can be observed at the level of the jowls, malar area, and mandibular border. B: Fifteen days after treatment, with specific improvements in the indicated areas (own source).
In Figure 5, we observe clear improvements in skin quality at the periocular contour and in the midface.

Figure 5: 60-year-old female patient. A: Before treatment-specific points are visible, marked by the dotted arrow in the mid-third region. B: 15 days after treatment-specific improvements are evident in the marked areas.
Figure 6 Frontal view of a 54-year-old patient showing specific improvements, including in the nasolabial fold; although this was not a study variable, it is evident that the position of the tissues in the upper third indirectly influences the deepening of the nasolabial fold.

Figure 6: Female patient, 54 years old. A: Before treatment, specific points marked with the dotted arrow can be observed at the level of the midface. B: Fifteen days after treatment, with specific improvements in the indicated areas.
Conclusion
The combination of BTTA and HA is justified because the toxin reduces muscle contraction and the formation of dynamic folds, while the HA used in this study does not provide volume but instead improves dermal structure; together, they offer a more global rejuvenation of the midface and the face as a whole. The subdermal plane is a dynamic space where vessels, nerve endings, and collagen fibers that connect the dermis with the hypodermis converge. Application of Hialuxina (the proposed technique) enables direct interaction with the neurocutaneous system, which is responsible for controlling vascular tone, glandular secretion, and sensory perception. This route of administration makes local neurovascular regulation possible, which may explain the dermal changes observed. We recommend conducting further clinical studies and including more variables in order to achieve more robust verification of these findings.
References
- Al-Ashoor, W. M. J. (2025). Hybrid injection techniques in aesthetic medicine: Evaluating the clinical benefits of combining botulinum toxin and hyaluronic acid in upper face rejuvenation. International Journal of Innovative Research and Scientific Studies, 8(11):175-184.
Publisher | Google Scholor - Kircik, L., Goldust, M. (2025). The Role of Virtual and Augmented Reality in Advancing Drug Discovery in Dermatology. Journal of Cosmetic Dermatology, 24(2):e70071.
Publisher | Google Scholor - Liu, Y., Wang, L. (2025). A Randomized Controlled Trial of Botulinum Toxin Combined with Non-Cross-Linked Bovine Collagen for Improving Periorbital Wrinkles. Aesthetic Plastic Surgery, 49(24):6932-6941.
Publisher | Google Scholor - Moon, H., Fundaro, S. P., Goh, C. L., Hau, K. C., Paz-Lao, P., et al. (2021). A review on the combined use of soft tissue filler, suspension threads, and botulinum toxin for facial rejuvenation. Journal of Cutaneous and Aesthetic Surgery, 14(2):147-155.
Publisher | Google Scholor - Stuzin, J. M., Rohrich, R. J., Dayan, E. (2019). The facial fat compartments revisited: clinical relevance to subcutaneous dissection and facial deflation in face lifting. Plastic and Reconstructive Surgery, 144(5):1070-1078.
Publisher | Google Scholor - Yang, R., Bai, Y., Liu, C., Luo, J., Yang, Y., et al. (2025). Combination of Botulinum Toxin A and Hyaluronic Acid Improved Facial Pore Enlargement Caused by Acne. Journal of Cosmetic Dermatology, 24(4):e70198.
Publisher | Google Scholor - Issa, M. C. A., Fogaça, A., Palermo, E., Maluf, L., Ormiga, P., et al. (2023). Global facial rejuvenation using a new cohesive, highly concentrated hyaluronic acid filler: A descriptive analysis of 35 cases. Cosmetics, 10(4):105.
Publisher | Google Scholor - Bertossi, D., Giampaoli, G., Lucchese, A., Manuelli, M., Albanese, M., et al. (2019). The skin rejuvenation associated treatment—Fraxel laser, Microbotox, and low G prime hyaluronic acid: preliminary results. Lasers in Medical Science, 34(7):1449-1455.
Publisher | Google Scholor - Jiang, Y., Jiang, Y., Gao, Y., Yan, L., Zhao, D. (2025). The Comparative Study of the Effects of Botulinum Toxin Micro-Droplet Injection Combined with Micro-crosslinked Sodium Hyaluronate Gel or Focused Ultrasound Technology in Facial Rejuvenation Treatment. Aesthetic Plastic Surgery, 49(19):5284-5291.
Publisher | Google Scholor - Petchngaovilai, C. (2009). Midface lifting with botulinum toxin: intradermal technique. Journal of Cosmetic Dermatology, 8(4):312-316.
Publisher | Google Scholor - Kapoor, R., Shome, D., Jain, V., Dikshit, R. (2010). Facial rejuvenation after intradermal botulinum toxin: is it really the botulinum toxin or is it the pricks? Dermatologic Surgery, 36:2098-2105.
Publisher | Google Scholor - Safia, A., Abd Elhadi, U., Merchavy, S., Batheesh, R., Bathish, N. (2025). Efficacy and Safety of Hyaluronic Acid Fillers for Midface Augmentation: A Systematic Review and Meta-Analysis. Medicina, 61(10):1823.
Publisher | Google Scholor























