

Research Article
Fluoride-Based Interventions for White Spot Lesion Prevention in Orthodontics: Varnish Versus Fissure Sealant
1Health Research Center, Chamran Hospital, Tehran, Iran.
2Assistant Professor, Dept. of Pediatric Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Mohammadreza Kashefi Baher, Health Research Center, Chamran Hospital, Tehran, Iran.
Citation: Mohammadreza K. Baher, Kooshki F. (2025). Fluoride-Based Interventions for White Spot Lesion Prevention in Orthodontics: Varnish Versus Fissure Sealant, Dentistry and Oral Health Care, BioRes Scientia Publishers. 4(3):1-6. DOI: 10.59657/2993-0863.brs.25.049
Copyright: © 2025 Mohammadreza Kashefi Baher, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 24, 2025 | Accepted: July 10, 2025 | Published: July 16, 2025
Abstract
Dental caries are often present as white spot lesions (WSLs) in their early stages; a concern heightened during orthodontic treatment. This in vitro study was conducted using 60 caries-free premolars, aimed to compare different interventions in preventing WSLs around orthodontic brackets. Samples were divided into four groups: Control, Fluoride Varnish (FV), Fluoride-Releasing Fissure Sealant (FRFS), and Non-Fluoride Fissure Sealant (NFFS). Each group received respective treatments, and orthodontic brackets were bonded. Demineralization-remineralization cycles were applied, and enamel microhardness was measured at the end of the study using a Vickers microhardness tester. Statistical analyses were performed using one-way ANOVA and Tukey’s post hoc test. The FV and FRFS groups had significantly higher microhardness compared to other groups (P < 0.05). FV exhibited the highest microhardness. However, the NFFS group did not significantly differ from the control group (P= 0.984). Overall, both FV and FRFS effectively reduce WSLs around orthodontic brackets.
Keywords: dental caries; orthodontic brackets; tooth demineralization; tooth remineralization
Introduction
Dental caries is one of the most common chronic oral diseases worldwide, presenting in its initial stages as white spot lesions (WSLs) [1,2]. Orthodontic treatments are a major contributing factor to the development of these lesions, as they make it challenging to maintain proper plaque control around the brackets and alter the microbial ecology [3-5]. The increased risk of demineralization during orthodontic treatment underscores the need for effective preventive measures. Fluoride application has long been established as one of the most effective methods in the prevention of dental caries, owing to its ability to promote enamel remineralization [6,7]. Various studies have recommended the use of fluoride in the form of either fluoride varnish or fissure sealant to combat caries development. Fissure sealants, especially those that release fluoride, are widely regarded as one of the most effective ways to prevent occlusal caries, as the fluoride they release helps to inhibit the growth of cariogenic bacteria like Streptococcus mutants, which are major contributors to caries development [8]. Fluoride varnish, on the other hand, has shown significant effectiveness in preventing demineralization and the formation of white spot lesions around orthodontic brackets. Numerous studies have demonstrated its ability to reduce the risk of white spot lesions in patients undergoing orthodontic treatment, establishing it as a strong preventive measure in this population [9-11]. The rationale for conducting this study stems from the high prevalence of white spot lesions in orthodontic patients and the well-established role of fluoride in caries prevention. While various studies support the use of fluoride-based treatments, there are conflicting results regarding the comparative efficacy of fissure sealants and fluoride varnish in preventing white spot lesions around orthodontic brackets. Therefore, this study aims to compare the effectiveness of these two preventive strategies, hoping to identify the most effective measure for reducing dental caries and improving oral health outcomes in patients undergoing orthodontic treatment.
Methods
Sixty healthy, caries-free premolars, extracted for orthodontic purposes from systemically healthy patients less than six months ago, were selected for this in vitro experimental study. The sample size was determined based on the study power of 0.8 and a type I error of 0.05, and the mean and standard deviation from a previous similar study [10], resulting in 15 teeth per group.
The teeth were stored at room temperature in normal saline, with the solution replaced every two weeks. Prior to the experiment, the teeth were thoroughly cleaned using pumice and a brush, and the crowns were separated from the roots using a high-speed turbine. A rectangular window (3 × 4 mm) was prepared on the middle third of the buccal surface, and the remaining surfaces were covered with acid-resistant nail varnish (Moda Nail Polish). The samples were then mounted in self-cure acrylic (Marlic, Iran) and coded from 1 to 60. Before starting the experiment, the microhardness of the enamel in the buccal surface of each sample was measured using a Vickers microhardness tester (Roell, Zwick, Germany) with a 200 N force applied for 10 seconds at three different points. The values were recorded in data forms for each sample.
The 60 samples were randomly divided into four groups:
- Control Group: No material was applied around the orthodontic brackets.
- Fluoride Varnish Group: 5% sodium fluoride varnish containing xylitol (Alvand Shimi, under license from VERICOM) was applied around the orthodontic brackets.
- Fluoride-Releasing Fissure Sealant Group: Fluoride-releasing fissure sealant (Pulpdent, Embrace Wetbond, USA) was applied around the orthodontic brackets and cured for 30 seconds.
- Non-Fluoride Fissure Sealant Group: Non-fluoride fissure sealant (Masterdent, Dentonics, USA) was applied around the orthodontic brackets and cured for 30 seconds.
The samples were dried, and acid etching and bonding were applied. Orthodontic brackets were then bonded to the center of the window on the buccal surface of each tooth.
To mimic the caries process, the teeth underwent cycles of demineralization and remineralization. The demineralization solution (pH = 4.5) and remineralization solution (artificial saliva, pH = 7) were prepared according to the following formulations [12,13]:
Demineralization Solution: CaCl2 (2.2 mM), NaH2PO4 (2.2 mM), Acetic acid (50 mM), NaCl (100 mM), NaF (1 ppm), NaN3 (0.02%).
Remineralization Solution: KCl (0.04%), NaCl (0.04%), CaCl2.2H2O (0.09%), NaH2PO4.2H2O (0.069%), MgCl2.6H2O (0.008%), Urea (0.05%), Ascorbic acid (0.01%), H2O (10 cc), Methyl-p-hydroxybenzoate (0.15%), PEG 6000 (7%), Glucose (0.1%).
Each tooth was immersed in the demineralization solution for 3 hours, followed by a brief rinse with distilled water. The teeth were then immersed in artificial saliva for 21 hours. This 24-hour cycle was repeated daily for 14 days, and all procedures were performed in an incubator at 37°C.
On the 14th day, the brackets were removed using a bracket remover plier without damaging the tooth structure. The materials applied around the brackets were also carefully removed. The microhardness of the enamel around the brackets in all four groups was then re-measured at three points around the bracket area using the Vickers microhardness tester under the same conditions as the initial measurements (200 N force, 10 seconds). The results were recorded in data forms for statistical analysis.
The mean and standard deviation of the microhardness values for each group were calculated separately. Comparative analysis between the groups was performed using one-way ANOVA test and p-value of less than 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS ver.29. The study was approved by the Ethical Committee of Shahid Beheshti University of Medical Sciences with the ethical code IR.SBMU.DRC.1397.057, ensuring adherence to all ethical considerations throughout the research process.
Results
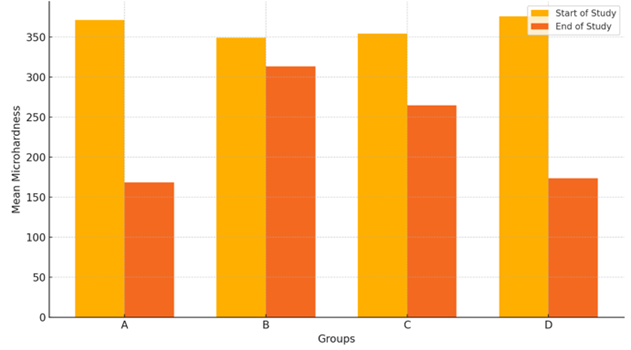
In this study, 60 premolar teeth were divided into four groups for comparative analysis. To assess the normality of data distribution and to select the appropriate statistical test, the Shapiro-Wilk and Kolmogorov-Smirnov tests were applied across all groups. Based on these normality tests, a significance level greater than 0.05 was observed in all groups, indicating a normal distribution of the data. Consequently, a one-way ANOVA was employed for comparative analysis. The obtained results indicated that, by the end of the study, at least one group exhibited a statistically significant difference from the others. Therefore, post hoc multiple comparisons between groups were subsequently conducted using Tukey’s test. The mean and standard deviation of enamel microhardness in the four groups at the start and end of the study are presented in Table 1.
Table 1: Mean and standard deviation of enamel microhardness in all groups at the start and end of the study.
| Group | Time | Mean (VHN) | Standard Deviation | Minimum (VHN) | Maximum (VHN) |
| Control | Start | 371.35 | 48.23 | 267.67 | 447 |
| End | 168.6 | 27.79 | 136 | 214.33 | |
| Fluoride Varnish | Start | 349.15 | 35.57 | 297.57 | 418 |
| End | 313.31 | 28.41 | 247.67 | 354.67 | |
| Fluoride-Releasing Fissure Sealant | Start | 354.35 | 27.59 | 310 | 417.33 |
| End | 264.66 | 47.18 | 177 | 331 | |
| Non-Fluoride Fissure Sealant | Start | 375.95 | 52.7 | 291.67 | 455 |
| End | 173.53 | 42.18 | 115 | 284 |
This table provides detailed information, including mean, standard deviation, and the range of values (minimum and maximum), for each group, allowing for a comprehensive comparison across conditions. Moreover, to visually highlight the comparative differences in mean microhardness values between the start and end of the study, a bar chart (Figure 1) is also included.
The comparison of enamel microhardness among the four groups at the start of the study revealed no statistically significant differences between groups (P-values range from 0.314 to 0.991) (Table 2).
Table 2: Comparison of enamel microhardness among all groups at the start of the study.
| Group | Comparison | P-value |
| A | vs. B | 0.480 |
| A | vs. C | 0.689 |
| A | vs. D | 0.991 |
| B | vs. C | 0.987 |
| B | vs. D | 0.314 |
| C | vs. D | 0.504 |
The comparison of enamel microhardness between the four groups at the end of the study indicated statistically significant differences between all groups (P-values range from lessthan 0.001 to 0.004), except between the control group and the non-fluoride fissure sealant group (P-value = 0.984) (Table 3).
Table 3: Comparison of enamel microhardness between all groups at the end of the study.
| Group | Comparison | P-value |
| A | vs. B | lessthan 0.001 |
| A | vs. C | lessthan 0.001 |
| A | vs. D | 0.984 |
| B | vs. C | 0.004 |
| B | vs. D | lessthan 0.001 |
| C | vs. D | lessthan 0.001 |
Discussion
The findings of the present study demonstrate that conventional (non-fluoride) fissure sealant had minimal impact in preventing caries, underscoring the critical role of fluoride in caries prevention. Our results showed significantly higher enamel microhardness around orthodontic brackets in the fluoride varnish and fluoride-releasing fissure sealant groups compared to the control group, indicating substantial effectiveness in preventing early caries initiation in the form of WSLs around brackets. In contrast, non-fluoride fissure sealant did not significantly differ from the control group in terms of enamel microhardness, which suggests that fluoride presence is a key factor in enhancing microhardness and resisting demineralization.
These findings align with the study by Layane et al., which reported a 58% reduction in the risk of WSLs around orthodontic brackets in patients using fluoride-releasing materials compared to those not using fluoride products [14]. Additionally, Demito et al. observed a 38% reduction in caries depth in patients treated with fluoride varnish versus the control group [11]. The study by Mary et al. also supports these findings, showing reduced demineralization in groups treated with fluoride-releasing composites [15]. Moreover, Sardana et al. emphasize the importance of effective at-home plaque control using fluoride-containing products during orthodontic treatment [16].
Conversely, the study by Benham et al. indicated that non-fluoride fissure sealant could significantly increase the risk of WSL formation in orthodontic patients [17]. However, in the present study, the non-fluoride fissure sealant group showed no significant impact on enamel microhardness, likely due to the sealant's protective barrier, which may suffice in limiting WSL formation in the short term. Differences in results could stem from in vitro conditions and shorter study durations in our experiment compared to the Benham et al. study.
The mechanism by which fluoride reduces WSLs and dental caries can be summarized as follows:
- Incorporation into enamel structure, increasing resistance [18].
- Enhancement of remineralization [19].
- Inhibition of demineralization [19].
Suppression of cariogenic bacteria through various mechanisms, including the reduction of acid production [20,21].
As such, fluoride-containing materials are recommended for patients undergoing orthodontic treatment to maintain optimal enamel health.
Notably, our study found a statistically significant difference in enamel microhardness in favor of fluoride varnish over fluoride-releasing fissure sealant by day 14. This suggests that fluoride varnish may offer a more potent reduction in caries progression under similar conditions.
Fluoride varnishes such as Duraphat in Europe and Duraflur in the United States have been widely adopted due to their ease of application, efficiency in reducing fluoride ingestion, and suitability for children and individuals with special needs. Skold et al. found that fluoride varnish effectively reduced proximal caries and provided an economic advantage [22]. Likewise, Sonesson et al. conducted a systematic review and found that regular applications of fluoride varnish during orthodontic treatment with fixed appliances significantly reduced the prevalence of WSLs [23]. Furthermore, Hu et al. highlighted the effectiveness of remineralizing agents, including fluoride varnish, in preventing and treating orthodontically induced WSLs [24]. Consistently, Wadih et al. demonstrated that fluoride varnishes significantly reduced demineralization around, but not beneath, orthodontic brackets [10].
Perrini et al. also noted the positive impact of fluoride varnish in preventing WSLs, though the effect was comparable to regular oral hygiene practices [25]. Furthermore, He et al. reported that fluoride varnish effectively enhances remineralization [26]. Moreover, Li et al. compared fluoride varnish and fluoride-releasing fissure sealant, finding both effective in reducing caries without, however, a statistically significant difference [27]. Overall, various fluoride-based interventions can be effective; however, their clinical impact may somewhat depend on the amount of fluoride uptake by the dental structure [27,28].
Conclusion
Fluoride varnish and fluoride-releasing fissure sealant can significantly reduce the incidence of white spot lesions and caries around orthodontic brackets. Among these, fluoride varnish demonstrated superior effectiveness compared to fluoride-releasing fissure sealant. The primary function of non-fluoride fissure sealant appears to be limited to its sealing properties, without a notable effect on enamel microhardness. These findings suggest that fluoride-based interventions play a crucial role in caries prevention for orthodontic patients.
Declarations
Acknowledgements
None
Authors’ Contributions
MKB: Methodology, Investigation, Writing - Original Draft, Visualization.
FK: Conceptualization, Supervision, Data Analysis, Review & Editing.
Competing Interests
None.
References
- Arora, A., Evans, R. W. (2012). Is the Consumption of Fruit Cariogenic? Journal of Investigative and Clinical Dentistry, 3(1):17-22.
Publisher | Google Scholor - Kimura, T., Dunn, W. J., Taloumis, L. J. (2004). Effect of Fluoride Varnish on the In Vitro Bond Strength of Orthodontic Brackets Using a Self-Etching Primer System. American Journal of Orthodontics and Dentofacial Orthopedics, 125(3):351-356.
Publisher | Google Scholor - Chapman, J. A., Roberts, W. E., Eckert, G. J., Kula, K. S., González-Cabezas, C. (2010). Risk Factors for Incidence and Severity of White Spot Lesions during Treatment with Fixed Orthodontic Appliances. American Journal of Orthodontics and Dentofacial Orthopedics, 138(2):188-194.
Publisher | Google Scholor - Chin, M. Y., Sandham, A., Rumachik, E. N., Ruben, J. L., Huysmans, M. C. D. (2009). Fluoride Release and Cariostatic Potential of Orthodontic Adhesives With and Without Daily Fluoride Rinsing. American Journal of Orthodontics and Dentofacial Orthopedics, 136(4):547-553.
Publisher | Google Scholor - Boersma, J. G., Van der Veen, M. H., Lagerweij, M. D., Bokhout, B., Prahl-Andersen, B. (2005). Caries Prevalence Measured with QLF After Treatment with Fixed Orthodontic Appliances: Influencing Factors. Caries Research, 39(1):41-47.
Publisher | Google Scholor - Hengtrakool, C., Kukiattrakoon, B., Kedjarune-Leggat, U. (2011). Effect of Naturally Acidic Agents on Microhardness and Surface Micromorphology of Restorative Materials. European Journal of Dentistry, 5(1):89-100.
Publisher | Google Scholor - Tabatabaei Rad, A. S., Tavassoli-Hojjati, S., Hoda, R. S., Aghaei, S. (2025). Efficacy of Remineralizing Agents for Prevention of Microhardness Reduction and Change in Mineral Content of Enamel in Anterior Primary Teeth after Exposure to Iron Drop. Journal of Dentistry, 26(2).
Publisher | Google Scholor - Chang, H. S., Walsh, L. J., Freer, T. J. (1997). Enamel Demineralization during Orthodontic Treatment. Aetiology and Prevention. Australian Dental Journal, 42(5):322-327.
Publisher | Google Scholor - Dawes, C. (2003). What is The Critical pH and Why Does a Tooth Dissolve in Acid? Journal-Canadian Dental Association, 69(11):722-725.
Publisher | Google Scholor - Abou Hamdan, W., Badri, S., El Sayed, A. (2018). The Effect of Fluoride Varnish in Preventing Enamel Demineralization Around and Under Orthodontic Bracket. International Orthodontics, 16(1):1-11.
Publisher | Google Scholor - Demito, C. F., Vivaldi-Rodrigues, G., Ramos, A. L., Bowman, S. J. (2004). The Efficacy of a Fluoride Varnish in Reducing Enamel Demineralization Adjacent to Orthodontic Brackets: An In Vitro Study. Orthodontics & Craniofacial Research, 7(4):205-210.
Publisher | Google Scholor - Bakhsh T, Al-Batati M, Mukhtar M, Al-Najjar M, Bakhsh S, et al., editors. (2018). Lasers in Dentistry XXIV, 24th Edition, SPIE - International Society for Optics and Photonics, San Francisco, California, United States, 2-3.
Publisher | Google Scholor - Pereira, A. D. F. F., Silva, T. C. D., Silva, T. L. D., Caldana, M. D. L., Bastos, J. R. M., et al. (2012). Xylitol Concentrations in Artificial Saliva After Application of Different Xylitol Dental Varnishes. Journal of Applied Oral Science, 20:146-150.
Publisher | Google Scholor - Nascimento, P. L. D. M. M., Fernandes, M. T. G., Figueiredo, F. E. D. D., Faria-e-Silva, A. L. (2016). Fluoride-Releasing Materials to Prevent White Spot Lesions Around Orthodontic Brackets: A Systematic Review. Brazilian Dental Journal, 27:101-107.
Publisher | Google Scholor - Melo, M. A., Morais, W. A., Passos, V. F., Lima, J. P., Rodrigues, L. K. (2014). Fluoride Releasing and Enamel Demineralization Around Orthodontic Brackets by Fluoride-Releasing Composite Containing Nanoparticles. Clinical Oral Investigations, 18:1343-1350.
Publisher | Google Scholor - Sardana, D., Schwendicke, F., Kosan, E., Tüfekçi, E. (2023). White Spot Lesions in Orthodontics: Consensus Statements for Prevention and Management. The Angle Orthodontist, 93(6):621-628.
Publisher | Google Scholor - Benham, A. W., Campbell, P. M., Buschang, P. H. (2009). Effectiveness of Pit and Fissure Sealants in Reducing White Spot Lesions During Orthodontic Treatment: A Pilot Study. The Angle Orthodontist, 79(2):338-345.
Publisher | Google Scholor - Mehta, A. (2013). Biomarkers of Fluoride Exposure in Human Body. Indian Journal of Dentistry, 4(4):207-210.
Publisher | Google Scholor - Featherstone, J. D. (1999). Prevention and Reversal of Dental Caries: Role of Low-Level Fluoride. Community Dentistry and Oral Epidemiology, 27(1):31-40.
Publisher | Google Scholor - Hamilton, I. R. (1990). Biochemical Effects of Fluoride on Oral Bacteria. Journal of Dental Research, 69(2_suppl):660-667.
Publisher | Google Scholor - Mortazavi, M., Kohanteb, J., Jahanimoghaddam, F. (2007). Inhibitory Effects of NaF-Varnish and APF-Gel on Cariogenic Bacteria: An In Vitro Study. Journal of Dentistry, 8(2):64-73.
Publisher | Google Scholor - Sköld, U. M., Petersson, L. G., Birkhed, D., Norlund, A. (2008). Cost-Analysis of School-Based Fluoride Varnish and Fluoride Rinsing Programs. Acta Odontologica Scandinavica, 66(5):286-292.
Publisher | Google Scholor - Sonesson, M., Twetman, S. (2023). Prevention of White Spot Lesions with Fluoride Varnish During Orthodontic Treatment with Fixed Appliances: A Systematic Review. European Journal of Orthodontics, 45(5):485-490.
Publisher | Google Scholor - Hu, H., Feng, C., Jiang, Z., Wang, L., Shrestha, S., et al. (2019). Effectiveness of Remineralising Agents in Prevention and Treatment of Orthodontically Induced White Spot Lesions: A Protocol for A Systematic Review Incorporating Network Meta-Analysis. Systematic Reviews, 8:1-11.
Publisher | Google Scholor - Perrini, F., Lombardo, L., Arreghini, A., Medori, S., Siciliani, G. (2016). Caries Prevention during Orthodontic Treatment: In-Vivo Assessment of High-Fluoride Varnish to Prevent White Spot Lesions. American Journal of Orthodontics and Dentofacial Orthopedics, 149(2):238-243.
Publisher | Google Scholor - He, T., Li, X., Dong, Y., Zhang, N., Zhong, Y., et al. (2016). Comparative Assessment of Fluoride Varnish and Fluoride Film for Remineralization of Postorthodontic White Spot Lesions in Adolescents and Adults Over a 6-Month Period: A Single-Center, Randomized Controlled Clinical Trial. American Journal of Orthodontics and Dentofacial Orthopedics, 149(6):810-819.
Publisher | Google Scholor - Li, F., Jiang, P., Yu, F., Li, C., Wu, S., et al. (2020). Comparison between Fissure Sealant and Fluoride Varnish on Caries Prevention for First Permanent Molars: A Systematic Review and Meta-Analysis. Scientific Reports, 10(1):2578.
Publisher | Google Scholor - Navabi, B., Ansari, G., Khan, Z., Kheirieh, P., Najafi, B. (2011). Fluoride Uptake Level of the Enamel by a Fluoride Varnish and a Fluoride Gel (APF). Journal of Dentistry, 12(3):214-220.
Publisher | Google Scholor























