

Case Report
Facial Adipo-Structuring Technique Quantified by Facial Scanner, Comparison of Results with Cadaveric Structures
1University Center Uningá, Parana, Brazil.
2CEO US University, Bogotá, Colombia.
3Centro Latinoamericano de Entrenamiento Médico e Investigación (CLEMI), Bogotá, Colombia.
*Corresponding Author: Gladys Velazco, Centro Latinoamericano de Entrenamiento Médico e Investigación (CLEMI), Bogotá, Colombia.
Citation: Rivera M, Arana G, Blanco R, Velazco G. (2025). Facial Adipo-Structuring Technique Quantified by Facial Scanner, Comparison of Results with Cadaveric Structures, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 5(1):1-8. DOI: 10.59657/2997-6103.brs.25.111
Copyright: © 2025 Gladys Velazco, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 18, 2025 | Accepted: December 04, 2025 | Published: December 12, 2025
Abstract
Health sciences have experienced rapid technological advancement, enabling successful treatments in various areas. In the field of orofacial harmonization, a specialty that converges between medicine and dentistry, numerous alternatives have been developed to address aging. Among these, facial adipo-structuring stands out, an innovative technique that intelligently addresses fat pads, relocating structures through cellular stimuli that activate collagen production. This process impacts all layers of the skin, generating beneficial changes. The main objective of this clinical case was to describe the adipo-structuring technique in detail and evaluate its results using the facial scanner, a novel tool for obtaining precise and comprehensive measurements. The research was conducted on a 59-year-old male patient, selected for presenting signs of aging associated with weight loss. Facial scans were performed before the start of treatment and after each phase of facial adipo-structuring. The results showed significant changes in the patient's face from the first phase of treatment. Improvements in skin texture, reduction of facial volume, tissue repositioning, and increased skin brightness were observed. It is concluded that the adipo-structuring technique is effective for rejuvenation and the facial scanner is a precise tool that provides three-dimensional results.
Keywords: facial adipo-structuring; orofacial harmonization; cellular senescence; facial scanner; aging
Introduction
The facial adipo-structuring technique represents a significant challenge in the management of soft tissues in the area of orofacial harmonization. This challenge lies in ensuring the replacement of fat pads through the application of senolytic agents that enable a change in skin structures, such that changes can occur from very obvious to subtle and may go unnoticed by the naked eye. Therefore, the application of a precision facial scanner tool, from the beginning to the end of treatment, allows for a more complete evaluation of the results obtained during the process and aids in accurate and objective interpretation [1]. Among the various available evaluation techniques, the use of the facial scanner stands out among other existing evaluation methods, considering its use within current technological advances [2]. Similarly, the facial adipo-structuring technique presents itself as a promising, innovative, and conservative treatment for cellular rejuvenation. This is why the various techniques offered in orofacial harmonization are chosen for the presentation of a clinical case. It is considered a technique that generates an "intelligent rejuvenation" named in honor of its author [1].
As a growing number of health professionals adopt this technique in clinical practice, more detailed follow-up methods are suggested, from the initial application to the delivery of immediate results. Clinical photography and facial scanners are valuable aids due to their precision, as they also guarantee an objective evaluation in the delivery of the results obtained. In this context, the before and after clinical photograph is the primary option for initiating treatment due to its easy access [3]. However, the facial scanner presents itself as an ideal alternative, as it allows for three-dimensional observation of results. Although its high cost can be considered a disadvantage, as it is not accessible to most professionals [2]. It is worth noting that adipo-structuring is an unprecedented technique with excellent clinical results, generally documented by digital photographs [1]. The objective of this clinical case was to detail the facial rejuvenation technique with adipo-structuring, observing the alterations through the facial scanner, as an [11] innovative alternative to evaluate the results accurately, objectively, and completely, with the aim of obtaining detailed information about skin structures [12].
A detailed understanding of the skin and its structure, as well as the aging process, is fundamental to addressing facial rejuvenation techniques. In this theoretical framework, not only the anatomy of the skin and the alterations it undergoes over time are explored, but also the various strategies used to reverse or mitigate the effects of aging [4]. From ancient practices to the most recent advances in biotechnology, the search for "eternal youth" has led to the evolution of various facial rejuvenation techniques. Examining these practices leads to the research done by Velazco [1], called facial adipo-structuring, as a procedure that has stood out in the field of aesthetic medicine. In addition to its theoretical foundations, a separate chapter of a clinical case will be presented, which will be evaluated through clinical photographs and facial scanners for the traceability of the process applied to a specific patient [1]. Present the scientific basis behind facial adipo-structuring and explore how modern technologies, such as facial scanning and the traditional use of clinical photographs, are integrated into clinical practice to objectively establish the results of these facial rejuvenation processes. The detailed analysis of these aspects provides a more complete understanding of the technique and the changes in the rejuvenation process [5,6].
Facial anatomy, essential for discovering the complex morphophysiological alterations associated with the aging process, presents a multi-layered structure that plays a fundamental role in the appearance and functionality of the face. These layers, interconnected and with specific functions, are distributed from the outermost surface to the deepest layers, collectively influencing facial dynamics and their evolution over time [7]. In the second layer, the subcutaneous tissue and superficial adipose tissue house fat compartments that go beyond simple fat storage. These fat pads not only contribute to facial volume but also play a crucial role in the structural support of the skin, maintaining its elasticity and tone [7]. Russo and Loreto [7] highlight the importance of the fat pad as essential tissues that go beyond simple fat storage, contributing significantly to the structure and elasticity of the skin. However, a series of negative factors, such as weight gain and exposure to UV rays, can contribute to skin aging. Facial fat compartments are divided into two categories: mobile superficial fat and deep, immobile fat. The superficial compartments are distributed in the latero-temporal, central, and medial temporal cheek, forming different areas such as the infraorbital compartment, mid-cheek, nasolabial, central cheek, latero-temporal, and mandibular compartments. Each of these compartments has specific characteristics and is delimited by particular ligaments and anatomical structures [8]. For example, the infraorbital compartment, located in the tear trough, is limited by the orbicularis retaining ligament, known as McGregor's ligament, and is notable for its water retention capacity. The cheek is subdivided into medial, central, and latero-temporal compartments, each with defined locations and boundaries, such as the orbicularis ligament, zygomatic-cutaneous ligament, and parotid-cutaneous ligament. The mandibular compartment, the lower face compartment, is separated by the nasolabial compartment and is attached to the depressor anguli oris muscle, with boundaries defined by structures such as the depressor labii inferioris muscle and the platysma muscle [4]. These fat compartments and their anatomical characteristics are essential for understanding facial dynamics and the alterations associated with aging, providing valuable information for facial rejuvenation techniques and aesthetic procedures [9-14].
Scientific research has shown selective atrophy of the deep fat compartments and hypertrophy of the superficial fat compartments. In this sense, the lower face compartment group is separated by the nasolabial compartment and is attached to the depressor anguli oris muscle, with boundaries defined by structures such as the depressor labii inferioris muscle and the platysma muscle [4]. 59It is important to know that facial adipo-structuring is an innovative technique that involves the manipulation and reorganization of adipocytes and subcutaneous fat compartments in the face to restore or improve facial harmony and aesthetics and, due to its implications, possesses technical principles, which Cotofana et al. [4] studied in depth, managing to clarify the following technical principles: facial adipose anatomy: it is based on a deep knowledge of the topography and histology of facial fat compartments. These compartments, differentiated into superficial and deep, present significant individual variations in terms of volume and distribution [4]; dynamics of facial aging recognizes that facial aging is not attributable only to skin ptosis or dermal atrophy, but also to the redistribution, atrophy, and herniation of facial fat compartments and volumization and contouring techniques uses filling and modeling strategies to restore or enhance facial volume, employing techniques such as autologous lipo-structuring (fat transfer) and the use of biocompatible dermal fillers [5].
Also Cotofana et al. [5] explain that the application of the technique requires tools and applications, such as: fat micrograft cannulas allow the precise transfer of autologous adipocytes, favoring optimal integration and cell survival; 3D facial scanners and analysis software are used to map facial topography, allowing for detailed and personalized treatment planning; and biomedical imaging technologies such as high-resolution ultrasonography, to assess the distribution and quality of adipose and dermal tissues [5]. It is essential to understand that, in contemporary practice, facial lipo-structuring is applied not only in aesthetic contexts but also in post-traumatic reconstruction or the correction of congenital deformities, standing out for its minimally invasive approach and its ability to achieve natural and long-lasting results [34]. Adipo-structuring focuses on working with the existing anatomy in the patient. This involves relocating and optimizing adipose tissue without drastically altering the underlying facial structure [1], achieving rejuvenation from within. While procedures such as chemical peels or dermabrasion act on the surface of the skin, adipo-structuring acts at a deeper level, impacting the fat compartments for a more comprehensive and lasting rejuvenation (33). Similarly, Cotofana et al. [4] discusses advanced technology for facial analysis and, unlike traditional techniques that rely primarily on visual and manual evaluation, it often uses cutting-edge technology, such as 3D scanning and ultrasound for precise mapping of facial structure.
The facial adipo-structuring technique, in the context of aesthetic medicine and plastic surgery, involves several fundamental stages and considerations, reflecting its advanced and personalized approach [1]:
Evaluation and Planning Initial Consultation: A complete evaluation of the patient is performed, including their medical history, expectations, and aesthetic goals. The facial structure is analyzed using methods such as high-resolution photography;
Analysis of Fat Distribution: Specific areas where panicopathic restructuring can improve facial harmony are identified. This involves the evaluation of volume loss, tissue ptosis, and asymmetry. The patient is explained what is expected from the technique and the possible alternative treatments they may need in the future [1].
Procedure: The technique is explained to the patient, giving them the opportunity to ask questions and express any doubts they may have. Then, the treatment [1] is performed using the same clinical protocol that will be described in detail in the treatment phases below.
Post-Procedure and Recovery: Postoperative Care: Detailed instructions are given on the care of the treated areas; Follow-up: Recovery is not necessary, as the technique is not disabling, however it is necessary to warn the patient that they should not go to the beach, swimming pool, saunas, etc., [1].
Current Considerations: Personalization: Each procedure is tailored to the unique needs and characteristics of the patient, ensuring that the results are natural and harmonious with the overall facial structure [36].
Facial adipo-structuring, therefore, represents a fusion of artistic skill and technical precision, in addition to indispensable clinical care and biosafety to guarantee the success of the technique, providing an attractive option for those seeking facial rejuvenation with natural results [1].
Case Presentation
The clinical case of a patient in whom the facial adipo-structuring technique was used, aiming to describe the improvement in the physical appearance of typical signs of aging, such as tissue ptosis, appearance of nasolabial folds, glabellar lines due to gesticulation and permanent muscle contraction, in addition to thinning of the skin in some facial areas. All these alterations are associated with various factors related to aging.
A clinical case of a 57-year-old male patient is presented in whom the technique will be applied, documenting the process with clinical photographs before and after, as well as facial scan photos and their respective 3D prints to verify facial alterations favorable to facial rejuvenation. The importance lies in choosing the appropriate technique within a treatment plan, after evaluating the patient and performing a comprehensive diagnosis. The success of the procedure is guaranteed by a thorough analysis, obtaining the medical history, understanding the patient's needs, and drawing up a list of positive and negative aspects to manage solutions, using the techniques that will be implemented in the treatment plan. It is essential to explain to the patient that the changes will be progressive, will not depend solely on a single procedure or technique, and that maintenance protocols are imperative, possibly using various techniques in a single session or over several sessions.
To perform the clinical technique, three specific clinical steps are required: the first is the design of the fat pad map, which consists of a facial map formed directly by the location of the fat pads and their insertion points. A precise and accurate marking of each of the pads and the separation between them of the interceptal ligaments must be made, which are treated after the restructuring of the pads [1]. Facial planimetry is performed with the patient in an upright position, with the Frankfort plane parallel to the floor to facilitate the spatial observation of the facial pads. Then, using a marker, the facial planes begin to be positioned in relation to the real anthropometric and morphometric points present in the facial region as we see in figure 1.

Figure 1: Marking of the facial paniculopathic system, in cadaveric analogy showing the location of each one. Superficial facial dissection performed at the Centro Latinoamericano de Entrenamiento Medico e Investigación, CLEMI, Bogotá, Colombia.
After marking, topical anesthesia Benzocaine 20% is applied to the cannula entry sites to improve surgical management. The numbers used are 22 G x 40 mm for the fat pads and 27 G x 50 mm. The access opening is made with a larger gauge needle to begin the entry of the cannula in a torque movement, and the sculpting is performed with two cannular movements: torque and in-and-out simultaneously in each of them according to the number of marked vectors. It is recommended to perform the sculpting between three to five times and subsequently leave the active principle, which consists of a cocktail containing Centella asiatica, caffeine, Melilotus extract, pyruvic acid, organic silicon, and a Hexa peptide to avoid total lipolysis and maintain a balance with lipogenesis.
Once the fat pad treatment is completed, the interceptal spaces are continued to be treated with number 27 G X 50 mm cannulas, inserting them at 90 degrees and then, the plane is changed to 45 degrees, also changing the active principles to Dimethylaminoethanol (DMAE), organic silicon, and Hexa peptide number 38, injected only once and without rotation of the cannula, to generate synthesis of extracellular matrix and production of choline to improve nerve stimulus, improving the proprioceptive reflex [1] Figure 2.
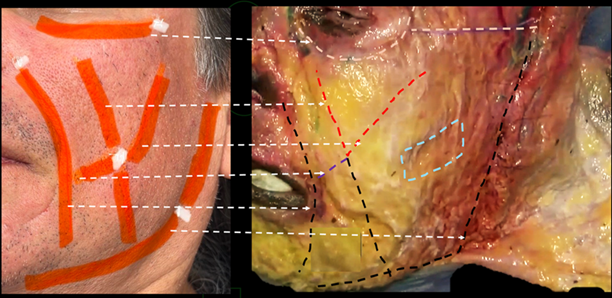
Figure 2: Anatomical relationship of the interceptal spaces in cadaveric analogy. Superficial facial dissection performed at the Centro Latinoamericano de Entrenamiento Medico e Investigación, CLEMI, Bogotá, Colombia.
Rigorous protocols and safe practices were established aimed at preserving the health and well-being of the patient. Aspects such as the sterilization of the work area, the hygiene of the environment, and measures to prevent possible complications during and after the procedure are addressed. Furthermore, it is considered that the training and qualification of the involved personnel guarantee the correct implementation of these measures. Protocols for the prevention of infections and complications are established; the technique has proven to be safe [38]. It is stated that adverse events related to the technique are very few and range from ecchymosis, pain on palpation, erythema, or moderate edema that resolve within a maximum of 72 hours; in less than 1% infections have occurred as a result of the required asepsis and antisepsis in the procedures. Therefore, it is necessary to address biosafety protocols in order to prevent infections.
Three sessions were repeated every 25 days and photographs were taken before and after treatment, in order to photographically verify the changes obtained.
The proposed photographic technique was through a facial scanner, Shining 3D Einstar facial scanner, which must be calibrated every time it is used, as the equipment includes its own software. The patient had to be positioned with a craniocervical support device located in the occipital region to prevent head movements. The facial scan began with an initial recognition of the patient's face so that the scanner detected the areas to be examined. Once the equipment recognized the superior, inferior, and lateral points during this process, the facial scanner moved from right to left and from top to bottom to copy all surfaces of the face.
The importance of traceability through monitoring the technique with photos and facial scans should be emphasized, as it provides a complete and objective view of the results obtained.
Subsequently, printing is done with gray Anycubic resin, photopolymerizable with an LCD light source for better printing with high precision, low shrinkage, and dimensional stability, resulting in a model with clear details.
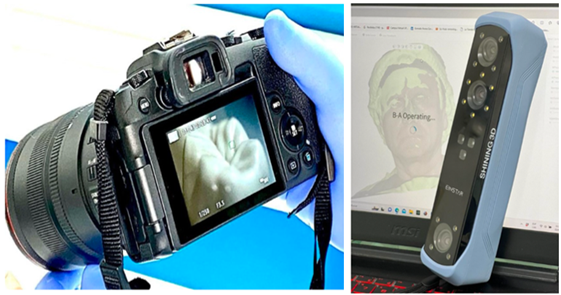
Figure 3: Canon RP macro 100 camera and Shining 3D Einstar facial scanner.

Figure 4: Printing with gray Anycubic resin, photopolymerizable with LCD light source, of the models obtained before and after treatment.
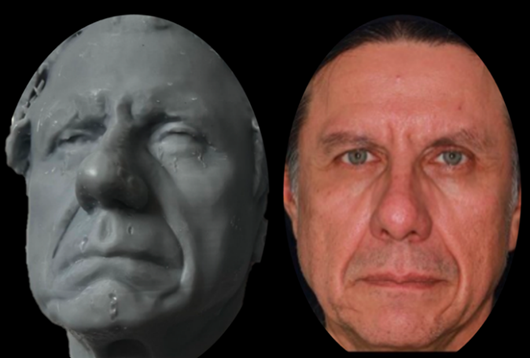
Figure 5: Comparative analysis of the 3D print with the patient's clinical photograph before treatment.
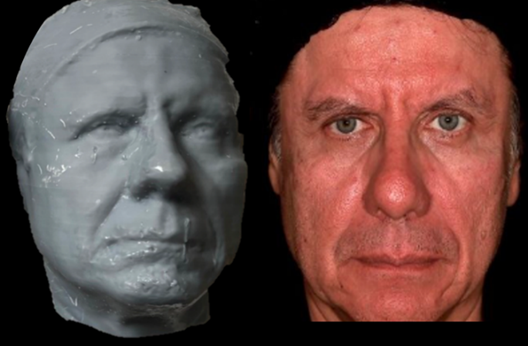
Figure 6: Comparative analysis of the 3D print with the patient's clinical photograph after treatment.
Results and Discussion
With the use of the standardized photographic protocol and the use of the facial scanner, it can be defined that the changes in the patient are detailed, even the most subtle ones, which can often go unnoticed by the visual evaluation of the observer, even the patient. The facial scanner is a precision technology that does not allow for erroneous results or results that can be altered due to its fidelity and non-manipulation. The 3D prints are faithful reprints of the real image of the model, which guarantees the obtaining of the changes achieved in the procedure. It is worth highlighting the fact that many fine details are imperceptible, but with this results validation technique we can obtain fidelity. If the photos are observed in comparison with the scans, it is verifiable that the improvement is much more exact in the models than in the photos themselves, which further strengthens the use of these tools for the verification of cases and their improvements.
Conclusion
The facial adipo-structuring technique has proven to be highly effective in tissue restructuring, preparing them in an optimized way for subsequent treatments or other orofacial harmonization techniques that seek to attenuate the signs of facial aging. Regarding the facial scanner, its relevance as a cutting-edge tool with significant technological advances is confirmed. Its ability to show facial alterations with a precision of up to 0.1 mm is essential for evaluating treatment results objectively and in detail. This allows us to recommend the tool as a diagnostic complement in clinical practice.
References
- Velazco G. (2020). Facial Adipo-structuring. Act Bioclinica. 10(20).
Publisher | Google Scholor - Martínez PP. (2022). Facial scanner: What advantages does it offer in dental treatments?
Publisher | Google Scholor - Pérez, J. C. G., Leal, Y. C. D., Barrios, V. S., Martínez, G. R., Chávez, L. S. (2019). The importance of clinical photography in dentistry. Archivos de Investigación Materno Infantil, 10(3):88-90.
Publisher | Google Scholor - Cotofana, S., Fratila, A. A., Schenck, T. L., Redka-Swoboda, W., Zilinsky, I., et al. (2016). The anatomy of the aging face: a review. Facial Plastic Surgery, 32(03):253-260.
Publisher | Google Scholor - Cotofana S et al. (2016). Anatomy of the Facial Fat Compartments in Cadaver Studies: A Systematic Review. Aesthetic Surgery Journal. (36):497-507.
Publisher | Google Scholor - Russo PR, Loreto F. (2021). The New Face from anatomy to aesthetic medicine. Amolca.
Publisher | Google Scholor - Kruglikov, I., Trujillo, O., Kristen, Q., Isac, K., Zorko, J., et al. (2016). The facial adipose tissue: a revision. Facial Plastic Surgery, 32(6):671-682.
Publisher | Google Scholor - Alghoul, M. S., Vaca, E. E., Mioton, L. M., Zins, J. E. (2020). The functional anatomy of the deep facial fat compartments: a detailed imaging-based investigation. Plastic and Reconstructive Surgery, 145(4):870e-871e.
Publisher | Google Scholor - de Oliveira, T. R. C., Pacheco, R. F., Cardoso, Á. L. (2023). Anatomia da face e processo de envelhecimento facial. Aesthetic Orofacial Science, 4(1):48-57.
Publisher | Google Scholor - Cotofana, S., Lachman, N. (2019). Anatomy of the facial fat compartments and their relevance in aesthetic surgery. JDDG: Journal der Deutschen Dermatologischen Gesellschaft, 17(4):399-413.
Publisher | Google Scholor - Chaudhri, S. K., Jain, N. K. (2014). History of cosmetics. Asian Journal of Pharmaceutics, 3(3).
Publisher | Google Scholor - Protasoni, M., Serrano, M. (2023). Targeting mitochondria to control ageing and senescence. Pharmaceutics, 15(2):352.
Publisher | Google Scholor - Ponce Alencastro, J. A. (2021). Envejecimiento: Consideraciones generales sobre sus teorías biológicas. Ciencia Latina Revista Científica Multidisciplinar. 5(1):140-164.
Publisher | Google Scholor - Mendelson, B., Wong, C. H. (2012). Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic plastic surgery, 36(4):753-760.
Publisher | Google Scholor - Navarrete-Reyes, A. P., Montaña-Álvarez, M. (2009). Inflammaging. Envejecimiento de origen inflamatorio. Revista de Investigación Clínica, 61(4):327-336.
Publisher | Google Scholor - Pires ASPR, Teuro SR, Pilon MD. (2023). Facial aging and orofacial harmonization - a narrative literature review. Research, Society and Development, 12(5), e15312541591.
Publisher | Google Scholor - Castilla Camacho, M. (2022). Armonización orofacial. Revista Estomatológica Herediana, 32(3):207-208.
Publisher | Google Scholor - Herrera, A., Soto Aguirre, N. (2022). Intelligent orofacial beauty: an epistemic reflection from the Venezuelan dental client. Ciencia ergo sum, 29(2).
Publisher | Google Scholor - Zaid, D. N. (2021). Non-Surgical Facial Rejuvenation Techniques (Doctoral dissertation, University of Zagreb. School of Medicine).
Publisher | Google Scholor - Barbosa, K. L., Furtado, G. R. D., Martin, E. E. B., Velença, J. L. B., da Silva Krause, R. G., et al. (2021). Diretrizes em harmonização orofacial para abordagem de tratamentos minimamente invasivos durante a pandemia COVID-19. Revista Eletrônica Acervo Saúde, 13(8):e8635-e8635.
Publisher | Google Scholor - Cohn, J. E., Greco, T. M. (2020). Advanced techniques for the use of neurotoxins in non-surgical facial rejuvenation. Aesthetic Plastic Surgery, 44(5):1788-1799.
Publisher | Google Scholor - Carbón, A. M. T., Vega, H. E., García, C. A. G., Aguilar, J. C. P., Aguirre, C. A. A., et al. (2021). Treatment Options for Facial Rejuvenation by Fillers. Acta Médica de Cuba, 22(2).
Publisher | Google Scholor - Siniscalchi SL, Teruo SR, Pilon MD. (2023). PRF in orofacial harmonization: a narrative literature review. Research, Society and Development. 12(6).
Publisher | Google Scholor - Pai, G. S. (2016). Complications in cosmetic dermatology: Crafting cures. JP Medical Ltd.
Publisher | Google Scholor - Lambros, V. (2007). Observations on periorbital and midface aging. Plastic and Reconstructive Surgery, 120(5):1367-1376.
Publisher | Google Scholor - Rohrich, R. J., Pessa, J. E. (2007). The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plastic and Reconstructive Surgery, 119(7):2219-2227.
Publisher | Google Scholor - Brown, B. (2022). The gifts of imperfection: Let go of who you think you're supposed to be and embrace who you are. Simon and Schuster.
Publisher | Google Scholor - Cash, T. F. (2004). Body image: Past, present, and future. Body Image, 1(1):1-5.
Publisher | Google Scholor - Al, A., Silvia, C. R., Albert, C., Guyuron, B., Chung, K. C. (2009). Plastic surgery: indications and practice. Elsevier Health Sciences.
Publisher | Google Scholor - Donofrio, L. M. (2000). Fat distribution: a morphologic study of the aging face. Dermatologic Surgery, 26(12):1107-1112.
Publisher | Google Scholor - Eid, L., Mao, X., Zhao, B., Mao, J., Qian, S., et al. (2023). Fat Compartment Gliding Theory–A Novel Technique for the Repositioning of Superficial Fat Compartments for Facial Rejuvenation. Clinical, Cosmetic and Investigational Dermatology, 3077-3090.
Publisher | Google Scholor - Ibarra, L., Camacho, R. (2023). Adipoestructuración facial: una nueva herramienta para la armonización orofacial. Secuencia de casos. Acta Bioclinica, 13(26):95-115.
Publisher | Google Scholor - Guevara, V. G., Viloria, G. J. V. (2023). Evaluando la eficacia y seguridad de la técnica de adipoestructuración facial: a propósito de una serie de casos. Acta Bioclínica, 13(25):56-71.
Publisher | Google Scholor - Pereira, F. F., Braga, C. T., Souza, M. S., Souza, D. M. (2021). Camadas da face e mudanças associadas com o envelhecimento facial. Aesthetic Orofacial Science, 2(2):129-143.
Publisher | Google Scholor - Hernández SR, Fernández CL, Baptista CM. (2018). Research Methodology Mexico: McGraw-Hill.
Publisher | Google Scholor - Yannas, I. V., Burke, J. F. (1980). Design of an artificial skin. I. Basic design principles. Journal of Biomedical Materials Research, 14(1):65-81.
Publisher | Google Scholor - Shiffman MA, Giuseppe AD. (2016). Liposuction: Principles and Practice. Springer-Verlag ed.
Publisher | Google Scholor - Pu, L. L. (2018). Fat grafting for facial rejuvenation and contouring: a rationalized approach. Annals of Plastic Surgery, 81(6S):S102-S108.
Publisher | Google Scholor























