

Research Article
Evaluation of CA 15-3 And CEA Tumour Markers in The Early Detection of Breast Cancer
- Horice Butao *
Swami Vivekanand Group of institutes, Banur, Punjab, India.
*Corresponding Author: Horice Butao, Swami Vivekanand Group of institutes, Banur, Punjab, India.
Citation: Butao H. (2026). Evaluation of CA 15-3 and CEA tumour markers in the early detection of breast cancer. Journal of Cancer Management and Research, BioRes Scientia publishers. 4(1):1-5. DOI: 10.59657/2996-4563.brs.26.025
Copyright: : © 2026 Horice Butao, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 16, 2026 | Accepted: May 30, 2026 | Published: June 05, 2026
Abstract
The early detection of breast cancer remains a significant challenge within a clinical practice. This is mostly true in areas where access to advanced diagnostic tools is restricted. Cancer markers including Cancer Antigen 15 - 3 (CA 15-3) and Carcinoembryonic Antigen (CEA) are widely utilized in clinical oncology. However, their effectiveness in early-stage diagnosis remains uncertain. This study will evaluate the diagnostic performance of CA 15 - 3 and Carcinoembryonic Antigen in the early detection of breast cancer. Some studies indicate that while elevated levels of these markers may be observed in affecting individuals, their sensitivity in detecting the early stage of breast cancer is relatively low with moderate specificity. Therefore, the combined use of both markers demonstrates slight improvement in diagnostic accuracy but remains insufficient as a standalone screening approach. Some factors like Tumor heterogeneity and biological variability further limit their clinical utility in early diagnosis. These results highlight the need for integrated diagnostic approaches that integrate tumor markers, imaging and various laboratory techniques to improve early detections and patient prognosis.
Keywords: breast cancer; CA 15 - 3; carcinoembryonic antigen; tumour markers; early detection; diagnostic accuracy
Introduction
Breast cancer is now the most common cancer in women worldwide and has become a challenge to public health systems around the world. Despite advances in medical technology and therapeutic interventions, breast Cancer still remains a major cause of morbidity and mortality especially in poor countries mostly in Africa and some middle-class countries where access to early diagnostic services is limited. The effectiveness of disease management is highly dependent on early detection which significantly improves prognosis, increases treatment effectiveness and reduces mortality rates.
Breast Cancer is a disease that develops from uncontrolled growth of abnormal cells in breast tissue driven by genetic mutations and complex biological processes. The heterogeneity of tumour types and disparity of disease progression makes early diagnosis challenging and often results in late detection and presentation at an advanced stage. Standard diagnostic procedures including imaging techniques such as, (i) mammography and (ii) Ultrasound. Histopathological examination is a significant step in the identification of disease. However, availability, cost and technical expertise may limit these methods, especially in resource limited settings and therefore there is a need to explore alternative diagnostic strategies.
Of the developing approaches, the use of serum tumour markers has gained attention because of their non-invasive nature and potential clinical utility. In the field of oncology, tumour markers such as Carcinoembryonic Antigen and Cancer Antigen 15 - 3 are frequently used to monitor disease progression and response to therapy. But their role in early-stage detection of breast cancer is still under discussion because these biomarkers may be elevated in some patients and their sensitivity in detecting early disease is relatively low and also their diagnostic reliability is affected by tumour heterogeneity, biological variability and patient specific factors.
The limitations of existing diagnostic tools coupled with the increasing burden of breast Cancer highlight the need for affordable cost effective and reliable means for early detection. The clinical usefulness of the most commonly used tumour markers such as CA 15 - 3 and CEA should be assessed in order to determine their possible contribution to early diagnosis, especially in areas where sophisticated diagnostic facilities are lacking. A full understanding of their diagnostic performance can lead to improved screening strategies and improved patient management.
This research paper explores the access to diagnostic performance of CA 15 - 3 and Carcinoembryonic Antigen (CEA) for early breast cancer detection. Specifically, is to determine levels of these tumour markers in affected individuals to assess sensitivity and specificity in early-stage disease and to compare their effectiveness when used individually and in combination. In the pursuit of these aims this study will contribute to the ongoing efforts to improve the early detection strategies and reduce the global burden of breast cancer.
Role of Tumour Markers in Breast Cancer

Figure 1: main tumour markers in human breast cancer
(Source: Nolan E, et al,2023)
Tumour markers are very important in diagnosing, monitoring and managing breast cancer. These biomarkers are mostly substances that are secreted by tumour cells or by the body in response to cancer development. In breast cancer tumour markers are frequently found in blood, serum or tissue samples and they do provide valuable clinical information about disease progression and therapeutic response.
One of the most studied tumour markers in breast cancer is Cancer Antigen 15 - 3 and
Carcinoembryonic Antigen. Despite though there's also another tumour marker called Human Epidermal Growth Factor Receptor 2 (HER2). CA 15 - 3 is a mucin glycoprotein of breast epithelial cells and is commonly elevated in patients with advanced stage of breast cancer. An increased CA 15 - 3 level may reflect tumour load and disease recurrence. CEA is also a glycoprotein involved in cell adhesion and elevated in several malignancies including breast cancer. CEA is not specific but when used together with other tumour markers it is useful in monitoring disease progression.
Another important biomarker associated with aggressive phenotype of breast Cancer is HER2. HER2 overexpression results in increased proliferation and poor clinical outcomes. Identification of HER2 positivity has dramatically improved breast cancer management with targeted therapies such as trastuzumab and pertuzumab.
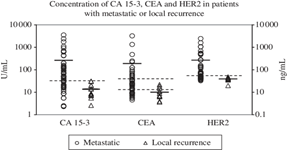
Figure 2
Source:https://www.researchgate.net/publication/235603976_Sensitivity_of_CA_15-3_CEA_and_serum _HER2_in_the_early_detection_of_recurrence_of_breast_cancer
Tumour markers are especially useful in assessing treatment response and tumour recurrence after therapy. Serial measurements of CA 15 - 3 and CEA levels can help clinicians to follow the changes of tumour activity during chemotherapy, radiotherapy or hormonal therapy. But these markers are not very sensitive for early breast cancer and so are not useful as a single test for screening.
The use of tumour markers together with imaging techniques such as mammography, ultrasound and magnetic resonance imaging (MRI) improves diagnostic accuracy and enhances early detection.
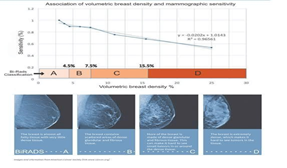
Figure 3
Source: https://www.cancer.org/cancer/breast-cancer/screening-tests-and-early-detection/mamm ograms/dense-breast-tissue.html
Progress in molecular diagnostics and genomic profiling continue to increase the role of biomarkers in personalized medicine, helping to improve patient outcomes and targeted therapeutic strategies.
Diagnostic Challenges in Early Detection of Breast Cancer
Even though there have been great developments in diagnostic techniques and screening programs, the early detection of breast cancer is still a big problem in clinical oncology. Low sensitivity of conventional tumour markers at the initial stages of disease development is one of the main problems of early breast cancer diagnosis. Biomarkers like CA15 - 3 and CEA are often elevated in advanced or metastatic breast cancer but may be normal in early tumour formation. Therefore, exclusive reliance on tumour markers may result in delay in diagnosis and reduced efficiency of treatment.
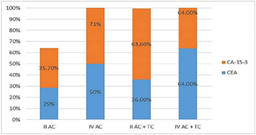
Figure 4: Comparison of diagnostic sensitivity of CA 15-3 and CEA in breast cancer patients.
One of the major challenges in early diagnosis of breast cancer is the low sensitivity of conventional tumour markers in the early stage of disease development. Tumour markers are frequently elevated in advanced stage of breast cancer but may be normal during the early formation of the tumour. Hence, relying solely on tumour markers may lead to a delayed diagnosis and decreased treatment efficiency.
Another big challenge is biological heterogeneity in subtypes of breast cancer. Different molecular subtypes including Luminal A, Luminal B, HER2 positive and Tripple Negative Breast Cancer (TNBC) have distinct biological behaviour and gambling odds. For instance, TNBC is a breast cancer that doesn't have Estrogen receptor (ER), Progesterone receptor (PR) and HER2 expression making early diagnosis and targeted treatment more difficult. Social economic and health care disparities also contribute to delayed breast cancer diagnosis especially in low- and middle-income countries. Poor access to screening facilities, lack of awareness programmes and shortage of trained healthcare personnel and poor diagnostic infrastructure have a huge impact on the rates of early detection and increase mortality.
They are some of the new technologies that hold promise to overcome current diagnostic problems such as;
- Liquid biopsy
- Circulating Tumour DNA (ctDNA)
- AI assisted imaging
- Multi Biomarker panels
These new approaches could enhance sensitivity, specificity and personalized risk assessment, thus improving early detection and clinical outcome.
Global Trends and Clinical Applications of Breast Cancer Tumours
Breast cancer is still the cause of many deaths in women all over the world. This has led to people using tumour markers like CA15-3 and CEA for finding, tracking and planning treatment for breast cancer. The number of breast cancer cases is rising globally. Doctors are relying more on these markers to help them. Breast cancer is a major problem and tumour markers are helping doctors to diagnose and treat it. The use of CA15-3 and CEA markers are becoming more common in breast cancer care.
The United States, Canada and other European countries have systems to check for breast cancer and they have the latest machines to diagnose it. This means that breast cancer is usually found early in these countries. On the other hand, many countries in Africa and Asia do not have it so good. They have a time because they do not have enough places to get checked for breast cancer and their hospitals are not well equipped. Such countries like Malawi, Zambia, Mozambique, Zimbabwe, Sudan, Somalia, Tanzania and other African countries. Though
Malawi has just built one of the modern Cancer hospitals (International Blantyre Cancer) in Blantyre still more it's lacking some of the equipment that can help to detect early breast Cancer among women. This often means that breast cancer is mostly found late in these countries. The USA, Canada and other European countries are really good at finding breast cancer at an early stage but many countries in Africa and Asia are still struggling with this.
Tumour markers help doctors a lot in treating patients. They are used to check if a treatment is working to find out if a tumour is growing back and to guide treatments. For example, HER2 testing has made a difference in treating patients with HER2 targeted drugs like trastuzumab. The HER2 test results helps doctors to decide if HER2 targeted therapy is right for patients with HER2 tumors. This HER2 testing has led to treatment outcomes for patients with HER2 positive cancer.
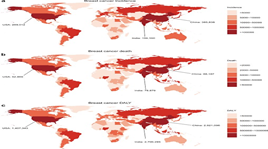
Figure 5: Global distribution of breast cancer incidence and mortality demonstrating regional disparities in disease burden and outcomes.
Source: world health organisation https://gco.iarc.fr/
Recent advances in molecular diagnostics, genomic profiling and liquid biopsy technologies continue to improve the accuracy and effectiveness of breast cancer management. These developments support personalized medicine and may help improve survival rates globally.
Limitations and Future Perspectives of Tumour Markers in Breast Cancer
Breast Cancer is a thing and tumour markers are really important when it comes to managing it. The thing is that these markers have some problems. For example, CA 15 - 3 and CEA may not go up when breast cancer is just starting. This means that they are not very good at the helping us to find the cancer in early stage. Sometimes these markers will go up when someone does not have cancer which can give us answers. Tumour markers like CA 15 - 3 and CEA are just not perfect. Breast cancer tumour markers are still useful. We need to be careful with them. Another problem with this is that breast cancer tumours are not all the same. Different types of breast cancer produce patterns of biomarkers. This makes it hard for one tumour marker to give correct diagnosis for breast cancer. Breast Cancer is a big concern and tumour markers, for breast cancer are not perfect.
Future perspectives focus on developing biomarkers using technologies like liquid biopsy. These technologies also include genomic profiling, artificial intelligence. Using many Biomarkers together. The goal is to improve how we detect breast cancer early. This can help make treatment more personalized. Better detection and treatment can lead to results for patients with breast cancer. The focus is on improving breast cancer management. Biomarkers will play a role in this. Breast cancer management will benefit from these advances.
Conclusion
Breast cancer is still a problem for people’s health around the world. Tumour markers like CA 15 - 3 and CEA and HER2 are important for breast cancer. They help doctors keep an eye on the disease and figure out what might happen. They also help doctors plan the treatment for breast cancer. These breast markers are not perfect. It is hard to find breast cancer early with them. When doctors use these breast cancer markers with other tests like imaging and molecular diagnostics, they can make better decisions and take better care of people, with breast cancer.
Advances in technology like biopsy, genomic profiling and artificial intelligence keep improving how we diagnose breast cancer and create personalized treatment plans. Early detection is crucial. More people need to know about breast cancer. We also need to make health care services more accessible. These are key to reducing breast cancer deaths around the world. Liquid biopsy and genomic profiling help doctors find breast cancer earlier. Artificial intelligence helps make sense of all the data. This means doctors can create treatment plans that are tailored to each patient. Early detection and awareness are vital. Many people do not have access to healthcare services. This can lead to detection and poor outcomes. Improving access to healthcare us essential. It can help reduce breast cancer mortality rates. Breast cancer is a health concern. It affects people worldwide. Advances in technology give us hope for diagnosis and treatment.
References
- World health organisation. (2023) Breast cancer fact sheets and global statistics. Geneva, Switzerland
Publisher | Google Scholor - International Agency for Research on Cancer. (2022) Global cancer Observatory: Breast Cancer Statistics
Publisher | Google Scholor - American Cancer Society. (2023) Breast cancer facts and figures
Publisher | Google Scholor - National Cancer Institute. (2021) Breast Cancer tumour markers
Publisher | Google Scholor - Centers for Disease Control and Prevention. (2022). Breast Cancer awareness and screening
Publisher | Google Scholor - Duffy MJ. (2006). Serum tumour markers in breast cancer are they if clinical value? Clinical chemistry,52(3), 345 - 351
Publisher | Google Scholor - Hayes DF. (1996). Tumour markers for breast cancer. Annals on Oncology,7(2) 185 - 190.
Publisher | Google Scholor - Harris L., et al., (20027). American society of clinical Oncology update of recommendations of the use of tumour markers in breast cancer. Journal of clinical Oncology
Publisher | Google Scholor - Molina R, et al., (2010). Tumour markers in breast cancer. Tumour biology,31(3) 165-173
Publisher | Google Scholor - Nicolini A, et al., (2013). The role of tumour markers in breast cancer. Biomedicine and
Publisher | Google Scholor - Bast RC jr. (2001). Status of tumour markers in ovarian and breast cancer patients. International journal of biological markers
Publisher | Google Scholor - Ali HQ. (2015). Evaluation of CA 15 - 3 and CEA in breast cancer patients. Medical Journal of
Publisher | Google Scholor - Park BW. et al., (2008). Prognostic utility of CA15-3 and CEA, Breast cancer research and treatment
Publisher | Google Scholor - Cristofanilli M., et al (2004). Circulating tumour cells and disease progression. New England journal of Medicine, 351 (8) 781 - 791
Publisher | Google Scholor - Breast cancer prognostic classification. Breast Cancer Research,12(4),207
Publisher | Google Scholor - Perou CM. et al., (2000). Molecular portraits of human breast tumours. Nature, 406(6797) 747-752
Publisher | Google Scholor - Heterogeneity in breast Cancer. Journal of clinical investigation, 121 (10), 3786 - 3788
Publisher | Google Scholor - Wan JCM., et al (2027). Liquid biopsies come of age. Nature reviews Cancer ,17(4) 223 - 238
Publisher | Google Scholor - Detection of circulating tumour DNA in early and late-stage malignancies. Science
Publisher | Google Scholor - Esteca A., et al. (2019). Deep learning for breast cancer diagnosis. Nature medicine 25(1),24-29
Publisher | Google Scholor - McDonald ES., et al. (2016). Breast imaging update: Mammography and MRI. Cleveland
Publisher | Google Scholor - Hanahan D., & Weinberg RA. (2011) Hallmarks of Cancer: The next generation cell ,144(5), 646-674
Publisher | Google Scholor























