

Case Report
Cor Triatriatum Sinister: A Rare Congenital Cardiac Defect in an Adult Treated by Surgical Correction with a Minimally Invasive Approach-A Case Report
- Sultan Sarwar Parvez 1*
- Mesbah Uddin 1
- Muhammad Sharif Hasan 2
- Mahamudul Hasan 2
- Prasanta Kumer Chanda 3
1 Associate Consultant, Department of Cardiac Surgery, Square Hospitals Limited, Dhaka, Bangladesh.
2 Specialist, Department of Cardiac Anaesthesia, Square Hospitals Limited, Dhaka, Bangladesh.
3 Senior Consultant, Department of Cardiac Surgery, Square Hospitals Limited, Dhaka, Bangladesh.
*Corresponding Author: Sultan Sarwar Parvez, Associate Consultant, Department of Cardiac Surgery, Square Hospitals Limited, Dhaka, Bangladesh.
Citation: Sultan S. Parvez, Uddin M., Muhammad S. Hasan, Hasan M, Prasant K. Chanda. (2025). The Utility of Computed Tomography in Estimating Ancestry, Journal of BioMed Research and Reports, BioRes Scientia Publishers. 8(4):1-6. DOI: 10.59657/2837-4681.brs.25.193
Copyright: © 2025 Sultan Sarwar Parvez, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 08, 2025 | Accepted: August 22, 2025 | Published: August 29, 2025
Abstract
Cor triatriatum sinister is a rare congenital cardiac defect where the left atrium is divided by a fibromuscular membrane in to two chambers: (a) a proximal chamber and (b) a distal chamber. It usually occurs in infancy or early childhood but is rare in adult hood. The gold standard for diagnosing cor triatriatum sinister is transthoracic echocardiography. Corrective surgery is the preferred choice of treatment. Traditionally, a standard median sternotomy is used to surgically treat the cor triatriatum. However, because of its cosmetic benefits, reduced pain, quicker recovery, and shorter hospital stay, the minimally invasive method is currently preferred over the traditional way.
Keywords: cor triatriatum sinister; congenital; heart defect
Introduction
Cor triatriatum sinister is a rare congenital acyanotic cardiac disease where the left atrium is divided by a fibromuscular membrane into two chambers:
a) a proximal or upper chamber and (b) a distal or lower chamber. The proximal chamber receives all pulmonary veins, and the distal chamber communicates with the mitral valve and left atrial appendage, called the ‘true’ atrium [1]. Cor triatriatum sinister was first reported by Andral and Church in 1868, although it was a post-mortem diagnosis [2]. The incidence of cor triatriatum sinister is 0.1% of clinically diagnosed and 0.4% of autopsy cases of all congenital cardiac diseases. Cor triatriatum sinister may be associated with other congenital cardiac anomalies like ostium secundum type of atrial septal defect (ASD), unroofed coronary sinus, and anomalous pulmonary venous drainage [3]. It usually occurs in early infancy or early childhood but is rare in adulthood. The clinical manifestation of cor triatriatum sinister depends on the size of the orifice in the membrane, which is permeated by one or more small perforations or orifices, allowing blood flow directly from the proximal to distal chamber, and the presence of other associated congenital cardiac anomalies. During infancy and early childhood, most of the patients present with dyspnea and pulmonary congestion [4]. However, in adults, the clinical appearance resembles that of mitral stenosis. Even so, some patients might not exhibit any symptoms until adolescence or even late adulthood.
Adults are more likely to have dyspnea, hemoptysis, and orthopnea due to heart failure, pulmonary venous/arterial hypertension, and obstruction of the pulmonary venous drainage. In addition, systemic thromboembolism due to intra-atrial thrombus formation and cardiac arrhythmias (extrasystole or atrial fibrillation) may cause palpitations [5,6]. Transthoracic color doppler echocardiography is an essential diagnostic tool. Surgical excision of fibromuscular membrane is the definitive choice of treatment. The conventional median sternotomy technique is used to surgically treat the cor triatriatum, although nowadays, minimally invasive techniques are preferred because of their cosmetic benefits, reduced pain, quicker recovery, and shorter hospital stays. Herein, we report a case of cor triatriatum sinister, a rare congenital cardiac defect in an adult that was treated surgically with a minimally invasive cardiac surgery (MICS) approach.
Case Presentation
A 29-year-old lady got admitted to our cardiac surgery unit through the outpatient department as a diagnosed case of cor triatriatum sinister to undergo surgery. She had a history of shortness of breath and fatigue, especially on exertion, since childhood, but before admission to the hospital, for the last two months, she experienced on & off chest pain for which she consulted with a physician and was advised to do an echocardiography, which revealed cor triatriatum sinister, and was advised for surgical correction. She was normotensive and nondiabetic. She was newly married. She had no history of fever, cough, hemoptysis, syncopal attack, or palpitation. She also had no previous history of cerebral stroke, bronchial asthma, chronic obstructive pulmonary disease (COPD), or heart disease in the family.
On physical examination, she was ill looking and did not have any cyanosis. Her pulse rate was 92 beats/min, blood pressure was 110/70 mmHg, and she had a normal respiratory rate with SpO2 of 97% at room air. On auscultation, the P2 component of the second heart sound was loud, and there was a systolic murmur in the left lower sternal area, no added sound in both lung fields. There was no hepatomegaly, distended veins, or neurological deficit. All biochemical reports showed normal. An electrocardiogram showed sinus tachycardia. Chest x-ray P/A view showed increased pulmonary vascularity.
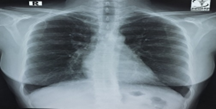
Figure 1: CXR P/A view showed increased pulmonary vascularity.
Echocardiogram revealed an oblique band like structure in LA about 16mm away from MV lateral annulus with 06 × 05 mm orifice suggest cor triatriatum sinister, a possible cleft at A2 of elongated AML causing mild MR, no supra mitral ring noted, dilated LA, PASP-35mmHg, no gross regional wall motion abnormality, normal LV systolic function (EF- 55%), no pericardial effusion was seen.

Figure 2: A transthoracic echocardiogram (Apical 4- chamber view) showed an oblique band-like membranous structure divided the LA, representing cor triatriatum sinister.
CT pulmonary angiogram with heart and great vessel showed prolapse of the anterior leaflets with membrane obstructions consistent with cor triatriatum and visualization of an accessory chamber that receives four pulmonary veins and communicates with the left atrium.
Then the patient was scheduled for surgical repair after evaluation. Written informed consent was obtained from the patient and her parents. Surgery was performed with endotracheal intubation using double lumen tube, single lung ventilation under G/A with a minimally invasive approach. Right lateral mini thoracotomy was done through the 4th intercostal space. Incision was about 4-5 cm in length. Pericardiotomy was done. Heparin was given. Right femoro-femoral bypass established after achieving ACT. An aortic cross clamp (CYGNET Flexible Clamp) was applied. Cold blood cardioplegia was delivered to arrest the heart at diastole. LA-tomy done.

Figure 3: Approach through Left atriotomy (Right lateral mini thoracotomy was done through the 4th intercostal space, CYGNET Flexible aortic cross clamp was applied, left atriotomy done)
After opening of the left atrium, the upper chamber was identified as containing four pulmonary veins. The upper and lower chambers were separated by a thick membrane containing two pin holes through which they were communicating. The membrane was excised, and the lower chamber was identified as containing the LA appendage and mitral valve.

Figure 4: Resection of membrane.
The LA appendage was plicated to prevent further formation of thrombus. Mitral valve patency was checked. LA tomy was closed.
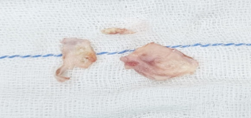
Figure 5: Specimen of resected fibromuscular membrane.
The Aortic cross-clamp was released after proper deairing. The patient was weaned from CPB to normal sinus rhythm. Decannulation was done after protaminization. The total aortic cross- clamping time was 50 min, and the total CPB time was 84 min for this patient. After maintaining proper hemostasis, the chest and femoral wound were closed in layers, keeping the RV pacing wire and right pleural drain tube in situ.

Figure 6: Right lateral thoracotomy (through 4th intercostal space) wound closure.
The postoperative course of the patient was uneventful. The patient was discharged from the hospital on the 6th postoperative day.
Follow-up
The patient was in good health at the one-month and three-month follow-ups, and a transthoracic color Doppler echocardiogram revealed no evidence of remnant of membrane throughout the LA.
Discussion
Cor triatriatum sinister is a rare congenital cardiac malformation, with about o.1-o.4% of among congenital heart defects. In adults, as cor triatriatum sinister is an extremely rare a condition, it has not drawn much attention in the literature. In adult patients, diagnosed with cor triatriatum sinister was a rare entity until the end of the 19th century, but in the last 2 decades, multiple cases with COS have been reported, even in adults [7]. The embryogenesis of cor triatriatum sinister depends on some hypothesis. These hypotheses include (a) The malseptation hypothesis, which postulates an anomalous development of the atrial septum involving the septum primum (b)The malincorporation hypothesis suggests an incomplete incorporation of the common pulmonary vein into the left atrium [8]. However, the most widely accepted hypothesis is the malincorporation hypothesis, which holds that the common pulmonary vein fails to fuse with the left atrium, resulting in a fenestrated, incomplete, or complete septum [9]. Loffler first categorized cor triatriatum into three categories based on the number of openings in the left atrial membrane [10].
Currently the morphological classification of cor triatriatum is divided into three categories: Type A, or” classic” triatrial heart, consists of a proximal chamber receiving all four pulmonary veins and a distal chamber encompassing the left atrial appendage and the mitral valve; the two chambers communicate through one or more small perforations in the membrane. Depending on the presence and location of an atrial septal defect, it has two subtypes: subtype A1 (septal defect communicating with the proximal chamber) and subtype A2 (septal defect communicating with the distal chamber). Type B hearts are those with an enlarged coronary sinus that receives all four pulmonary veins in the form of total anomalous pulmonary venous drainage. Type C is an extremely rare variant in which the proximal chamber receives no pulmonary veins [11]. The clinical manifestation of cor triatriatum sinister depends on the number and size of the orifice in the membrane. During infancy and early childhood, most of the patients present with dyspnea and pulmonary congestion. However, in adults, due to the large foramen and lack of an intra-atrial pressure gradient, adults with the disease usually asymptomatic, but it may present with the clinical appearance resembles that of mitral stenosis. In adults with cor triatriatum sinister, palpitations, orthopnea, and exertional dyspnea are the most common symptoms. In rare instances, patients may present with uncommon symptoms such as cardiac arrhythmia or syncope. Khanra et al. reported a 45- year- old patient who presented with chest pain that resembled an acute myocardial infarction was later diagnosed with cor triatriatum sinister [12]. Transthoracic echocardiography is the diagnostic tool of choice. At first, Cor triatriatum sinister may be confused with pulmonary veins or dilated coronary sinus on echocardiography, or even malignancy or thrombosis. However, the diagnosis with echocardiography alone can be aided using contrast-enhancing agents during ultrasound or a careful examination of the lesion using color Doppler imaging.
Compared to transthoracic echocardiography, transesophageal echocardiography provides better visualization of the LA and its membrane, which helps with precise diagnosis [13,14]. Cardiac magnetic resonance (CMR) is also considered the gold standard for measuring chamber volumes and function to evaluate right ventricular overload. It can be used to determine whether thrombosis is present in the accessory chamber (due to slow flow) or rule out malignancy.
Cardioembolic stroke is a common finding in cor triatriatum sinister, and potential mechanisms of thrombus formation include higher prevalence of atrial fibrillation, stagnation of blood flow in the accessory chamber and paradoxical embolization because of an accompanying atrial septal defect [15]. The treatment for cor triatrium sinister depends on the clinical presentation and severity of symptoms. If a patient is asymptomatic and an atrial membrane is found incidentally without a pressure gradient, no treatment is required. The surgical excision of the fibromuscular membrane is the choice of treatment in patients with cor triatrium sinister with also severe obstruction, and this procedure has been shown to provide satisfactory short-term and long-term survival rates with a low chance of requiring redo-surgery in the future.
The size of the membrane orifice determines the prognosis for cor triatrium sinister. In Niwayama's study the average survival rate was 16 years when the opening was greater than 3 mm and 3 months when it was 3 mm [12].
The choice of surgical approach depended on the suspected morphology of the defect and on the presence or absence of associated cardiac anomalies. The right atriotomy approach was preferred in cases with an associated atrial septal defect. The left atriotomy was preferred in uncomplicated cases. At first, the left atrial chamber was entered superiorly and medially to the right pulmonary veins, and then the obstructing membrane was carefully excised but extreme caution should be taken to avoid damage to the mitral valve and the atrial wall. Traditionally, a standard median sternotomy is used to surgically treat the cor triatriatum. However, because of its cosmetic benefits, reduced pain, quicker recovery, and shorter hospital stay, the minimally invasive method is currently preferred over the traditional way. Here, our patient is a diagnosed case of cor triatriatum sinister, a rare congenital cardiac defect in an adult, who presented with shortness of breath & fatigue on exertion and chest pain and was treated surgically for the first time with a minimally invasive approach.
Conclusion
Cor triatriatum sinister is a rare congenital acyanotic cardiac malformation that rarely presents during adulthood, and in adults, the clinical presentation may vary and resemble that of mitral valve stenosis. Echocardiography is the diagnostic tool of choice, but cardiac MRI helps in finding detailed information on cardiac anatomy. Surgical correction is the treatment of choice with safe and excellent long- term results in adult age compared to surgery in childhood. Surgical excision of the membrane by a minimally invasive approach (MICS) is the alternative to the traditional method because of its good cosmetic result, less pain, faster recovery, and short length of hospital stays with more patient satisfaction.
Declarations
Acknowledgments
Not Applicable
Conflicts of interest
The authors declare that there are no conflicts of interest.
Funding
None
Ethics
Written informed consent was obtained from the patient.
Consent to Participate
The work was approved by all the authors for participation.
Consent to Publications
The work was approved by all the authors for participation.
References
- Sankhyan, L. K., et al. (2021). Surgical management of divided atrial chambers. Journal of Cardiac Surgery, 36(12):4267–4279.
Publisher | Google Scholor - Patel, S. V., et al. (2017). Cor triatriatum sinister – A rare finding in older adult. Annals of Cardiology and Cardiovascular Medicine, 1(1):1–3.
Publisher | Google Scholor - Nassar, P. N., & Hamdan, R. H. (2011). Cor triatriatum sinistrum: Classification and imaging modalities. European Journal of Cardiovascular Medicine, 1(3):84–87.
Publisher | Google Scholor - Saxena, P., Burkhart, H. M., Schaff, H. V., Daly, R. C., Joyce, L. D., & Dearani, J. A. (2014). Surgical repair of cor triatriatum sinister: The Mayo Clinic 50-year experience. Annals of Thoracic Surgery, 97(5):1659–1663.
Publisher | Google Scholor - Braulio, R., Gomes, C. F., & Andrade, R. A. (2007). Cor triatriatum with mitral insufficiency and atrial fibrillation in a 36-year-old man. Revista Brasileira de Cirurgia Cardiovascular, 22(2):259–260.
Publisher | Google Scholor - Park, K. J., Im, S. I., Jung, J. H., Hong, P. Y., & Park, Y. T. (2009). Adult cor triatriatum presenting as cardioembolic stroke. Internal Medicine, 48(13):1149–1152.
Publisher | Google Scholor - Van Praagh, R., & Corsini, I. (1969). Cor triatriatum: Pathologic anatomy and a consideration of morphogenesis based on 13 postmortem cases and a study of normal development of the pulmonary vein and atrial septum in 83 human embryos. American Heart Journal, 78(3):379–405.
Publisher | Google Scholor - Lalezari, M. L., et al. (2018). Concurrent cor triatriatum sinister and levoatriocardinal vein in an 11-year-old boy presenting with foudroyant pulmonary edema after appendectomy: A living tribute to the mal-incorporation theory. Anatolian Journal of Cardiology, 21(3):172–174.
Publisher | Google Scholor - Edwards, J. E. (1949). Unusual malformation of the left atrium: Pulmonary sinus. Archives of Pathology, 48(5):371–376.
Publisher | Google Scholor - Lam, C. R., Green, E., & Drake, E. D. (1962). Diagnosis and surgical correction of 2 types of triatrial heart. Surgery, 51(1):127–137.
Publisher | Google Scholor - Khanra, D., Saha, S., Roy, O., & Banerjee, R. D. (2019). Cor triatriatum sinister presenting with acute myocardial infarction. Journal of Practical Cardiovascular Sciences, 5(3):208–212.
Publisher | Google Scholor - Buchori, E., Arifin, D., & Hidayat, P. (2024). Cardiac MR imaging of cor triatriatum sinister in an elderly man: A rare case report. Radiology Case Reports, 19(6):1468–1471.
Publisher | Google Scholor - Alaloola, A. A. (2022). Do we really need a new classification for cor triatriatum sinister? Journal of Cardiac Surgery, 37(12):4534–4535.
Publisher | Google Scholor - Amara, R. S., Jamal, L. R., Haseeb, J. J., & Nazir, S. H. (2020). Cardioembolic stroke in a young male with cor triatriatum sinister: A case report. European Heart Journal – Case Reports, 4(2):1–6.
Publisher | Google Scholor























