

Research Article
Cancer Caregivers’ Quality of Life and Socioeconomic Wellbeing: A Cross-Sectional Study at Tertiary Care Academic Hospital in A Low Middle-Income Country
- Muhammad Ammar Dogar *
- Kashif Ali Sarwar
- Samreen Tariq
Combined Military Hospital, National University of Medical Sciences, Rawalpindi, Pakistan.
*Corresponding Author: Muhammad Ammar Dogar, Combined Military Hospital, National University of Medical Sciences, Rawalpindi, Pakistan.
Citation: Dogar MA, Sarwar KA, Tariq S. (2026). Cancer Caregivers’ Quality of Life and Socioeconomic Wellbeing: A Cross-Sectional Study at Tertiary Care Academic Hospital in A Low Middle-Income Country, Journal of Clinical Research and Clinical Trials, BioRes Scientia Publishers. 5(2):1-6. DOI: 10.59657/2837-7184.brs.26.068
Copyright: © 2026 Muhammad Ammar Dogar, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 03, 2026 | Accepted: April 24, 2026 | Published: June 01, 2026
Abstract
Introduction: Cancer is a chronic disease causing psychological, social and financial challenges, resulting in decreased quality of Life (QoL) of caregivers. In this study, we aim to assess the impact of cancer on caregivers’ QoL and their socioeconomic wellbeing.
Materials and Methods: A Cross-sectional survey performed on total 121 caregivers of cancer patients who visited a public sector teaching hospital in Pakistan from Jun to Dec 2024. Average participant age was 35.7±11.2 years and 68% were females. The caregiver QoL assessment used a validated 35-item cancer-specific instrument score (0 - 140) points, and Socioeconomic status (SES) was determined through modified Kuppuswamy scale.
Results: Our study showed that most caregivers belonged to lower SES with “Upper Lower Class (IV)” representing 62.0% of the sample, rest were "Lower Middle Class (III)” 24.0%, "Lower Class (V)” 9.9%, and “Upper Middle Class (II)” 4.1%. The mean QoL score was 92.7±20.5 points ranging from 48 to 133. The QoL scale achieved excellent internal consistency (Cronbach’s alpha = 0.917). SES class IV caregivers had a highest mean QoL scores of 95.3±19.1. Demographic data on SES class were non-significant (F=1.31, p=0.27). QoL had weak, nonsignificant associations with education, occupation, and income (p > 0.05). SES had no significant effect in Multivariate regression analysis.
Conclusion: Cancer caregivers have moderately impaired QoL which is indicative of burden of caring their loved ones. While we did not find high differences of QoL among caregivers of various socioeconomic strata, this may be because most caregivers had highly burdensome roles irrespective of SES.
Keywords: cancer caregivers, socioeconomic status, quality of life, low-middle income
Materials and Methods
This is a cross-sectional observational study conducted at a tertiary care public sector hospital in Rawalpindi, Pakistan. We consecutively interviewed primary caregivers of inpatients and outpatients with confirmed cancer from June 2024 to December 2024. Unpaid family members who provided most of the patient’s care were defined as caregivers. Caregivers included in study are aged ≥18 years, taking care of a diagnosed cancer patient for at least ≥1 month, and able to answer the questionnaire. Professional caregivers, individuals with cognitive impairment, and those caregivers who were unwilling for interview were excluded from the study.
Sample Size
Anticipation of a moderate correlation (r ≈ 0.30) between the effect size (f² ≈ 0.10) and the associated SES and QoL, α = 0.05, power = 80%, two-tailed test implies a sample size of ≈ 84. Given the need to permit subgroup analysis, we aimed to target ≥120 caregivers. Keeping this in view, 121 caregivers were interviewed, which meets the required number estimated.
Data Collection and Materials
Data was collected through the use of face-to-face interviews. The parts of the questionnaire were as follows: (1) Demographics: caregiver age, gender, relation to patient, and cancer type of patient. (2) SES assessment: An updated Kuppuswamy-like scale of head of household education, occupation, and family income was used to assign a socioeconomic class (I-V) [10]. The total was summed and scored for each domain and was classified as forming upper (I), upper middle (II), lower middle (III), upper lower (IV) or lower (V) socioeconomic class domains. In South Asia, it is used to measure material resources on this composite SES instrument. (3) Caregiver QoL: A 35-item Caregiver Quality of Life Index -Cancer (CQOLC) tool (an Urdu translation valid for local use) was used. A total score of 0 to 140 is obtained by scoring each item from 0 to 4. Negative items are reversed such that higher totals indicate better QoL. Example items (“I feel satisfied with my social activities” vs “It bothers me that my routine is altered”) can be used to easily represent different items in this context. Cronbach’s alpha was used to evaluate the internal consistency of the tool. Demographic data on SES class did not produce statistically significant results according to results from one-way ANOVA (F=1.31, p=0.27).
Statistical Analysis
Data was analyzed using Statistical Package for the Social Sciences (SPSS) v26. Caregiver demographics and SES, as well as derived QoL, were summarized using descriptive statistics (means ± SD, frequencies). Internal consistency of the QoL scale (Cronbach’s alpha) was tested. For inferential analysis, we used one-way ANOVA (QoL scores by SES category), Spearman correlation (QoL and ordinal SES variables), and t-tests (QoL by cancer type). A p-value less than 0.05 was considered significant.
Results
The sample included 121 caregivers (mean age 35.7 ± 11.2 years; 68 percentage female). Most patients were cared for by their spouses (41%) and children (34%). A modified Kuppuswamy scale to assign socioeconomic class was used where the education, occupation and family income of the head of the family were worked out Level of education varied: 37% had less than high school, 29% had intermediate, 14% were graduate or more, and 12% were not educated at all. The majority of the family heads were skilled or semi-skilled workers; 23% were unemployed. Sixty percent of families earned an income of less than 45>90,000 PKR per month. As expected, the majority of the caregivers ffell into lower SES classes. Upper Lower Class IV is 62.0%, Lower Middle Class III is 24.0%, Lower Class V is 9.9%, and Upper Middle Class II is 4.1% (Figure 1). No caregivers were in Class I. The distribution of SES is presented in Figure 1 and mean QoL by SES in Figure 2. Sample characteristic and scale score tables summarize the sample.
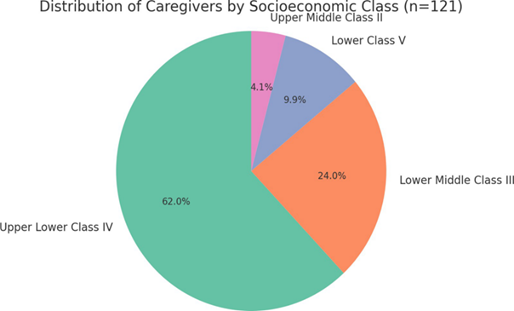
Figure 1: Distribution of caregivers by socioeconomic class (n=121). As shown, the predominant SES classes are Upper Lower (IV) and Lower Middle (III).
Overall, a mean caregiver QoL score of 92.7±20.5 (Range 48-133) was achieved. The CQOLC instrument had high internal reliability (Cronbach’s α=0.917). Main characteristics and scores by SES class are shown in Table 1.
Table 1: Distribution of Caregiver Quality of Life (QoL) Scores by SES Class (n=121).
| SES Class | Mean QoL Score ± SD |
| Class II | 90.6 ± 19.5 |
| Class III | 86.5 ± 22.0 |
| Class IV | 95.3 ± 19.1 |
| Class V | 92.3 ± 25.1 |
| Combined Mean | 92.7±20.5 |
Interpretation of QoL scores suggests a moderate caregiver burden. Class IV caregivers had a QoL score of 95.3±19.1, Class V 92.3±25.1, Class III 86.5±22 and Class II 90.6±19.5. Figure 2 illustrates these mean scores along with SD. As shown, there is no clear trend and the differences were not statistically significant.
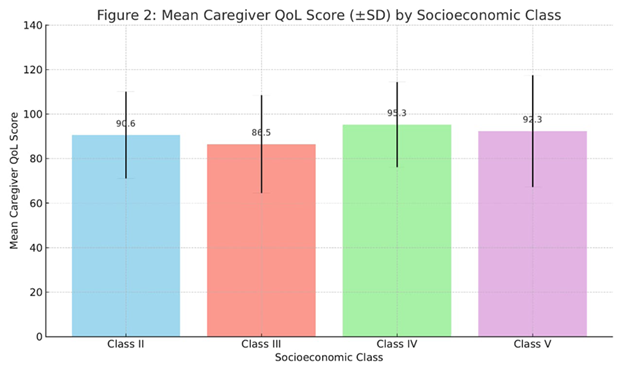
Figure 2: Mean caregiver QoL score (±SD) by socioeconomic class.
No significant association of QoL with SES was found by inferential tests. The value of F for the QoL by SES class one-way ANOVA was found to be F=1.31 with p=0.27. Similarly, Spearman correlation between QoL and the family income code (1-3) was weak (ρ=-0.082, p=0.38). There was no significant correlation with QoL (ρ≈-0.1, p>0.1) and educational level or occupation code, too. Notably, caregivers in lower SES did not report significantly worse QoL than their higher SES peers in this sample. QoL did not differ significantly by patient’s cancer type (mean 93.4 for solid tumors vs. 90.3 for hematologic, p=0.53) or gender (p=0.66). The high internal consistency (α > 0.9) indicates that the scale was validly measuring the construct in this cohort.
Discussion
We report on new data on cancer caregiver’s QoL and SES in a Pakistani oncology hospital setting. Caregivers (with a mean score of ≈93/140) generally did not have improved QoL compared to other studies reporting caregivers’ well-being as generally compromised [3,4,7]. However, contrary to our expectation, the QoL scores did not appear to be gradient with SES categories. In fact, our data showed that upper lower class (IV) caregivers reported slightly higher QoL than lower middle (III), though this finding was not statistically significant. It maybe that all our participants had limited circumstances, even that for the higher SES group was not wealthy, having indicated that cultural factors such as close family support may buffer SES effects.
This is in agreement with other studies in similar settings, where we also find modest QoL (approx. 93/140). For instance, there was a decline in psychosocial QoL and physical QoL dimensions as caregiver burden increased, as reported by Puia et al. [4]. Likewise, Singh et al. (India) found that caregivers in Class IV/V were subjected to greater financial burden when compared to caregivers in Class I/II [5]. The latter had somewhat lower QoL than the small high SES group (II), and there was a pattern of non-significant differences (consistent with the given); the lowest classes had somewhat lower QoL. Previous studies have noted that QoL in other studies tends to be better in higher SES caregivers [6]. Our study may not have been powered to detect modest SES effects, since we had only 5 caregivers in Class II. The care givers demonstrated moderate QoL deficits while SES indicators showed no substantial relationship with their care-related well-being in this participant collection.
Finally, our results in a global context are consonant with many others; caregivers often suffer anxiety, depression, and burden at rates much higher than their population in general [4]. Results from QoL indicate that about 30% of caregivers reported low scores under 70, which is associated with substantial distress. There is literature that indicates caregivers have depression rates of 25–40% and strong correlations between the burden of caregiver and poor QoL. As we did not actually assess depression, our QoL deficit probably represents that kind of mental health impact. Importantly, caregivers who are employed or who are educated have lower burdens and higher QoL than in Western countries [11], and this may possibly be related to coping resources and self-efficacy. Education and employment status were not found to significantly affect QoL, although the data for the variables were not available.
There may have been several factors that contributed to our null finding. It may be that cultural and family expectations in Pakistan lead to a floor effect, meaning almost all caregivers, across class, are very responsive. In addition, the composite SES measure may not fully encompass financial strains specific to caring (out-of-pocket costs, job loss). Yet, we did find that 89% of caregivers reported some income stress (consistent with other low-income settings), implying widespread financial burden. More studies could be done using detailed economic appraisal. These findings reflect the necessity to provide psychosocial support, counselling, and financial aid as such measures can help improve caregiver outcomes [12].
Strengths and Limitations: This study has used a validated caregiver QoL instrument and a standardized SES scale. Internal consistency (Cronbach’s α > 0.9) was also tested. The setting was a public sector hospital which is more reflective of prevailing scenario in our country, as majority of cancer patients are treated in public hospitals. However, limitations must be noted. The design is cross-sectional; therefore, causation is precluded. Subgroup analysis (only 5 in the highest SES) may be underpowered for our sample size (n=121). We did not have data on duration of caregiving or patients' performance status, which are known to affect caregiver QoL [2]. This was a single-center tertiary care hospital, which limits the generalizability of findings. For reasons of resource constraints, we were unable to additionally assess caregiver mental health (anxiety and depression scales), which may have enhanced understanding of determinants of QoL [13].
Conclusion
Our study concludes that caregivers have moderately impaired quality of life which is indicative of the great burden of caring for a loved one with cancer. While we did not find significant differences between QoL of caregivers in relation to socioeconomic strata as expected, this may be because most caregivers had highly burdensome roles irrespective of class. Routine caregiver well-being assessment by healthcare providers should be linked to providing families with the support services they need.
List of Abbreviations
QoL- Quality of Life
SES- Socioeconomic Status
SPSS- Statistical Package for The Social Sciences
CQOLC- Caregiver Quality of Life Index -Cancer Tool
Declarations
Acknowledgements
None.
Conflicts of Interest
Authors declared none.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Ethics Statement
The study protocol was ethically approved by Combined Military Hospital Ethics Review Committee (Ref: CMH/EC/03/2025). Participants consented to informed written consent. Confidentiality and voluntary participation were ensured in compliance with the Declaration of Helsinki. No violation of patient safety or privacy, breach of data, or human/institutional rights has been done.
Author Contributions
Muhammad Ammar Dogar: Conception and design, data collection, data interpretation and analysis, drafting, final approval.
Sidrah Tariq: Conception and design, data collection, Data interpretation and analysis, drafting, final approval.
Kashif Ali Sarwar: Conception and design, data interpretation and analysis, peer review, final approval.
Samreen Tariq: Conception and design, data collection, drafting, final approval.
References
- Zhai, S., Chu, F., Tan, M., Chi, N. C., Ward, T., et al. (2023). Digital Health Interventions to Support Family Caregivers: An Updated Systematic Review. Digital Health, 9:20552076231171967.
Publisher | Google Scholor - Alghamdi, W. A., Almatrafi, M. A., Asiri, R. A., Almuraee, L. A., Alsharif, S. M., et al. (2025). Quality of Life of Caregivers of Patients with Cancer: A Cross-Sectional Study. In Healthcare, 13(5):521.
Publisher | Google Scholor - García-Carmona, M., García-Torres, F., Jacek Jabłoński, M., Gomez Solis, A., Jaén-Moreno, M. J., et al. (2021). The Influence of Family Social Support on Quality of Life of Informal Caregivers of Cancer Patients. Nursing Open, 8(6):3411-3419.
Publisher | Google Scholor - Pop, R. S., Cojan Minzat, B. O., Ursu, C. P., Ursu, Ș., Puia, A. (2024). Decrease in Primary Caregivers’ Quality of Life During the Care of a Relative with Palliative Care Needs: A Prospective Longitudinal Study. Cancers, 16(21):3570.
Publisher | Google Scholor - Badger, T., Segrin, C., Crane, T., Morrill, K., Sikorskii, A. (2024). Social Determinants of Health, Psychological Distress, and Caregiver Burden Among Informal Cancer Caregivers of Cancer Survivors During Treatment. Journal of Psychosocial Oncology, 42(3):333-350.
Publisher | Google Scholor - Guerra-Martín, M. D., Casado-Espinosa, M. D. R., Gavira-López, Y., Holgado-Castro, C., López-Latorre, I., et al. (2023). Quality of Life in Caregivers of Cancer Patients: A Literature Review. International Journal of Environmental Research and Public Health, 20(2):1570.
Publisher | Google Scholor - Singh, K., Dogra, E., Pal, K. M., Negi, R. R., Vardhan, R., et al. (2023). Factors Impacting Quality of Life of Caregivers of Cancer Patients in The Sub-Himalayan Region: A Cross-Sectional Study. Cureus, 15(2).
Publisher | Google Scholor - Kondeti, A. K., Yadala, A., Lakshmi, N. R., Prakash, C. S. K., Palat, G., et al. (2021). Assessment of Caregiving Burden of Family Caregivers of Advanced Cancer Patients and Their Satisfaction with The Dedicated Inpatient Palliative Care Provided to Their Patients: A Cross-Sectional Study from A Tertiary Care Centre in South Asia. Asian Pacific Journal of Cancer Prevention: APJCP, 22(7):2109.
Publisher | Google Scholor - Arbani, S., Bibi, A., Hyder, S., Javed, S., Muhammad, T., et al. (2023). Assess the Burden of Caregivers of Cancer Patients at a Tertiary Care Hospital in Karachi, Pakistan: Burden of Caregivers of Cancer Patients. Pakistan BioMedical Journal, 37-41.
Publisher | Google Scholor - Mandal, I., Hossain, S. R. (2024). Update of Modified Kuppuswamy Scale for The Year 2024. Int J Community Med Public Health, 11(7):2945-2946.
Publisher | Google Scholor - Kuzu, F., Aydın, H. T. (2022). Effects of Education on Care Burden and Quality of Life to Caregivers of Patients with COPD. Turkish Thoracic Journal, 23(2):115.
Publisher | Google Scholor - Chow, R., Mathews, J. J., Cheng, E. Y., Lo, S., Wong, J., et al. (2023). Interventions to Improve Outcomes for Caregivers of Patients with Advanced Cancer: A Meta-Analysis. JNCI: Journal of the National Cancer Institute, 115(8):896-908.
Publisher | Google Scholor - Cui P, Yang M, Hu H, Cheng C, Chen X, et al. (2024). The Impact of Caregiver Burden on Quality of Life in Family Caregivers of Patients with Advanced Cancer: A Moderated Mediation Analysis of The Role of Psychological Distress and Family Resilience. BMC Public Health. 24(1):817
Publisher | Google Scholor























