

Case Report
Acute Pancreatitis as an Uncommon Manifestation of Systemic Lupus Erythematosus with Overlapping Sjögren’s Syndrome: A Case Report
1Postgraduate Resident in Internal Medicine, Universidad Internacional del Ecuador, Ecuador.
2Specialist in Internal Medicine, Universidad Internacional del Ecuador, Ecuador.
*Corresponding Author: Tannia Estefanía Aguirre-Soria, Specialist in Internal Medicine, Universidad Internacional del Ecuador, Ecuador.
Citation: Ramirez B.H.A., Soria T.E.A. (2025). Acute Pancreatitis as an Uncommon Manifestation of Systemic Lupus Erythematosus with Overlapping Sjögren’s Syndrome: A Case Report. Clinical Case Reports and Studies, BioRes Scientia Publishers. 10(1):1-6. DOI: 10.59657/2837-2565.brs.25.243
Copyright: © 2025 Tannia Estefanía Aguirre-Soria, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 12, 2025 | Accepted: March 26, 2025 | Published: April 02, 2025
Abstract
Lupus pancreatitis is a rare but potentially life-threatening complication requiring aggressive corticosteroid therapy for resolution. We present the case of a 22-year-old female with no relevant medical history who was admitted with persistent fever and a generalized rash, unresponsive to antibiotic therapy. As her condition progressed, she developed moderate epigastric pain, recurrent vomiting, and abdominal distension. The review of systems (ROS) revealed recent-onset polyarticular pain. On physical examination, she had a rash on the anterior chest, abdominal distension with diffuse tenderness, and within 24 hours, developed malar erythema and painful oral ulcers. Laboratory results showed pancreatic enzyme levels exceeding three times the upper limit of normal (ULN), leading to a diagnosis of acute pancreatitis. Extensive workup ruled out common causes, prompting an autoimmune evaluation, which confirmed systemic lupus erythematosus (SLE) with overlapping Sjögren’s syndrome (SS). The patient was started on high-dose intravenous corticosteroids (initially in pulses) and immunosuppressive therapy, leading to a gradual but complete clinical resolution. This case highlights an uncommon initial presentation of SLE, demonstrating the importance of considering autoimmune diseases in atypical pancreatitis cases. Recognizing these rare presentations allows for early diagnosis and appropriate immunosuppressive treatment, potentially improving patient outcomes.
Keywords: acute pancreatitis; systemic lupus erythematosus; sjögren’s syndrome; overlap syndrome
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder characterized by the production of autoantibodies targeting multiple organ systems, most commonly affecting the joints, skin, kidneys, and hematologic system. However, in rare cases, lupus-related immune complexes may deposit in pancreatic tissue, leading to localized vasculitis, thrombosis, and subsequent pancreatitis [1,2]. Lupus pancreatitis is a rare but severe complication, with an estimated prevalence of 1–5% [5,6]. The incidence is lower when it presents as the initial manifestation of SLE, making diagnosis particularly challenging. Additionally, SLE frequently coexists with other autoimmune conditions, with Sjögren’s syndrome (SS) being the most common, affecting up to 30% of lupus patients [3].
Lupus-related pancreatitis follows a more aggressive course than pancreatitis of other etiologies, leading to longer hospital stays, higher morbidity, and increased mortality [8,9]. Thus, early recognition is crucial, and treatment should be initiated promptly, guided by the predominant organ involvement. In cases of severe systemic inflammation with target organ damage, high-dose intravenous corticosteroids remain the cornerstone of therapy.
This report presents a rare case of acute pancreatitis as the initial manifestation of SLE with overlapping Sjögren’s syndrome. Given the lack of published cases in Ecuador, this case aims to raise awareness of atypical lupus presentations, encourage early diagnosis, and promote appropriate therapeutic management to improve outcomes.
Case Presentation
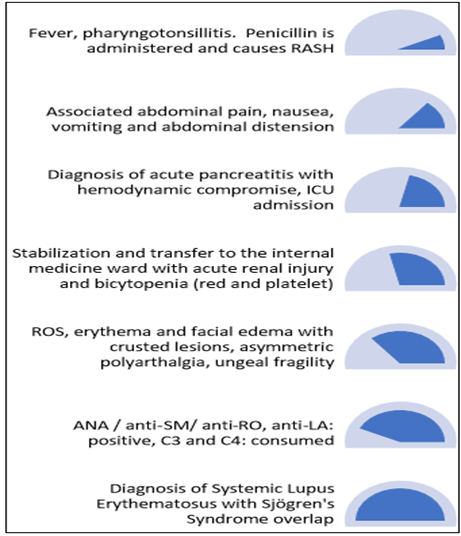
A 23-year-old female with no significant medical history or toxic habits, presented with a two-week history of fever, initially diagnosed as pharyngotonsillitis and treated with benzathine penicillin. She experienced a mild allergic reaction to the antibiotic without airway compromise. However, despite treatment, fever and malaise persisted, and after 48 hours, she developed mild, non-radiating epigastric pain, recurrent vomiting, and abdominal distension
On physical examination, notable findings included arterial hypotension, tachycardia, and fever recorded at 39.2°C (102.6°F). Additionally, there were blisters on the lower lip, maculopapular eruptions on the anterior and posterior thorax, and abdominal distension. Bowel sounds were diminished, and generalized abdominal tenderness was present on both superficial and deep palpation. Complementary laboratory tests (Table 1) revealed a threefold elevation of pancreatic enzymes, leading to the diagnosis of moderately severe acute pancreatitis.
Due to hemodynamic instability, the patient required admission to the intensive care unit for four days. An etiological workup was initiated by the primary care team, ruling out major causes. The patient was then transferred to the internal medicine ward, where further diagnostic evaluation continued. As part of the review of systems (ROS), the patient reported nail fragility, hair loss, intermittent asymmetric polyarthralgia affecting the metacarpophalangeal joints and knees, and a single episode of butterfly-shaped facial erythema two months prior. A repeat physical examination revealed disseminated crusted maculopapular lesions on the face, ischemic damage to the right earlobe, dry oral mucosa with inflammatory ulcers in the oral cavity (Images A and B), resolving maculopapular lesions on the thorax, and deep tenderness on palpation of the left flank and mesogastrium. Laboratory findings were significant for bicytopenia (mild normocytic normochromic anemia and mild thrombocytopenia), and acute kidney injury classified as KDIGO stage III.
Given the multisystem involvement—including gastrointestinal, dermatological, musculoskeletal, renal, and hematological manifestations—the differential diagnosis shifted toward a systemic autoimmune disorder, raising suspicion for systemic lupus erythematosus (SLE) with Sjögren’s syndrome overlap vs. medium-to-small vessel vasculitis. Additional immunological testing (Table 2) revealed positive autoimmune markers suggestive of SLE and SS, leading to the application of the SLICC/EULAR criteria and the Schirmer test (Table 3), both of which confirmed the suspected diagnosis. Ultimately, the case was concluded as acute pancreatitis as a manifestation of systemic lupus erythematosus with Sjögren’s syndrome overlap.
Diagnostic Assessment
Supplementary examinations
Table 1: Laboratory results. Hospital Padre Carollo “Un canto a la vida”
| Complete Blood Count | Blood Chemistry Panel | ||
| White blood cells | 4.72 K/uL | Lipase | 1990 (12N) |
| Neutrophils | 4.01 K/uL | Amylase | 1323 (10N) |
| Lymphocytes | 0.48 K/uL | Cholesterol | 96 |
| Hemoglobin | 11.6 g/Dl | Triglycerides | 180 |
| Hematocrit | 34.10% | AST | 15 |
| MCV | 87 fL | ALT | 8 |
| MCHC | 33.50% | Bilirubin total. | 0.29 |
| Platelets | 111.000 K/u | `Bilirubin direct | 0.23 |
| Bilirubin indirect | 0.05 | ||
| TSH | 4.47 | ||
| FT3 | 1.21 | ||
| FT4 | 0.905 | ||
| BUN | 52.5 | ||
| Creatinine. | 2.23 | ||
| Sodium. | 142 | ||
| Potassium | 4.7 | ||
| Chloride | 119 | ||
| Glucose | 92 | ||
| Total calcium | 8.9 | ||
Table 2: Laboratory results. Hospital Padre Carollo “Un canto a la vida”
| Autoimmune Markers | |
| ANA | 1:1280 |
| ANTI - CCP | 14.12 |
| Anti-SM | >300 |
| C3 | 19 |
| C4 | <2> |
| Anti-RO | >300 |
| Anti-LA | >300 |
| Anticardiolipin IGM | 3.50 |
| Anticardiolipin IGG | 12.60 |
| Anti-DNA DSS | 1394.31 |
| B2 Glycoprotein IGM | 1.90 |
| B2 Glycoprotein IGG | 6 |
| ANCA C | 2 |
| ANCA P | 0.90 |
| `IGG4 | 46.4 (3-201) |

Figure 1: Non-contrast and contrast-enhanced CT scan of the abdomen and pelvis
Transverse section: The pancreas is enlarged with a heterogeneous appearance, showing peripancreatic fat stranding suggestive of inflammation and fluid accumulation. There is associated free fluid in the peripancreatic region, with no areas of necrosis (Yellow arrows).
Table 3: Test Schirmer. Hospital Padre Carollo “Un canto a la vida”.
| Schrimer Test |
| Positive |

Figure 2: (A) Facial edema with widespread crusted maculopapular lesions across the face. (B) Erythematous papular lesion on the right earlobe with ischemic areas, showing a tendency toward necrosis.
Time Schedule
Therapeutic Intervention
Due to a high suspicion of systemic lupus erythematosus (SLE) and the absence of initial immunological results, it was decided to initiate corticosteroid pulse therapy with methylprednisolone at a dose of 1 gram intravenously daily for three days. This decision was made after ruling out infection and considering the severity of the case, which included significant dermatological involvement and suspected renal impairment. The regimen was subsequently transitioned to oral corticosteroids in combination with hydroxychloroquine 200 mg orally once daily and azathioprine.
Evolution
From the first day of pharmacological treatment, there was a progressive resolution of skin lesions, abdominal pain control, and recovery of renal function and hematologic parameters. The established treatment was maintained, and at the two-month follow-up, a complete resolution was noted. The patient exhibited total remission of dermatological lesions, absence of tenosynovitis or joint pain, normalization of nitrogenous waste levels, and resolution of cytopenia. The patient denied experiencing any adverse effects from the medication, and the current therapeutic regimen was continued.

Image 2: After 2 months of targeted treatment.
Discussion
Lupus pancreatitis is characterized by the deposition of antinuclear antibodies in the pancreatic parenchyma, leading to tissue inflammation [1,2]. Its global prevalence is rare, with an incidence ranging from 1% when it presents as the initial manifestation of the autoimmune disease to 5% when it occurs as a complication of previously diagnosed SLE. Nationally, there are no published studies on this condition, limiting data collection to understand its behavior within our population (5,6). Regarding its clinical presentation, it has been observed that lupus pancreatitis primarily manifests as acute pancreatitis. However, although less common, cases of chronic pancreatitis have also been reported [7].
Overlaps with other autoimmune diseases, such as systemic sclerosis, inflammatory myopathies, rheumatoid arthritis, and Sjögren’s syndrome, have been described. In the case of Sjögren’s syndrome, shared genetic markers, including IFI44L, ISG15, and ITGB2, have been identified. These genes activate molecular mechanisms related to interferon expression and cytokine-mediated signaling pathways, with reported international prevalence rates of 23
Conclusions
The presentation of an uncommon clinical case of SLE with overlap syndrome involving Sjögren’s syndrome contributes to a better understanding of the disease, facilitating a more accurate and timely diagnosis while optimizing medical resources. Additionally, the natural history of the disease provides clinical warning signs that should be carefully monitored to prevent adverse outcomes. Lastly, the prompt selection and initiation of appropriate treatment, guided by systemic involvement and current clinical guidelines, are essential for ensuring a favorable prognosis, as demonstrated in this case.
References
- Humberto, B.-O. L., Eduardo, M.-N., Alejandro, A.-M. M., & Alvaro y Valerdi-Contreras Lorena, L.-I. (s.f.). Pancreatitis aguda como presentación inicial de lupus eritematoso sistémico. Medigraphic.com.
Publisher | Google Scholor - Dima, A., Balaban, D. V., Jurcut, C., & Jinga, M. (2021). Systemic lupus erythematosus-related acute pancreatitis. Lupus, 30(1):5–14.
Publisher | Google Scholor - Gianordoli, A. P. E., Laguardia, R. V. R. B., Santos, M. C. F. S., Jorge, F. C., Da Silva Salomão, A., et al. (2023). Prevalence of Sjögren’s syndrome according to 2016 ACR-EULAR classification criteria in patients with systemic lupus erythematosus. Advances in Rheumatology, 63(1).
Publisher | Google Scholor - Cui, Y., Zhang, H., Wang, Z., Gong, B., Al-Ward, H., et al. (2023). Exploring the shared molecular mechanisms between systemic lupus erythematosus and primary Sjögren’s syndrome based on integrated bioinformatics and single-cell RNA-seq analysis. Frontiers in Immunology, 14.
Publisher | Google Scholor - Velasque Marques, E., Cerqueira Batista Filho, L. A., & Toledo Maciel, A. (2023). Acute pancreatitis caused by Systemic Lupus Erythematosus activity: A case report and literature review. Medwave, 23(07):e2684–e2684.
Publisher | Google Scholor - Breuer, G. S., Baer, A., Dahan, D., & Nesher, G. (2006). Lupus-associated pancreatitis. Autoimmunity Reviews, 5(5):314–318.
Publisher | Google Scholor - Wang, Q., Shen, M., Leng, X., Zeng, X., Zhang, F., & Qian, J. (2016). Prevalence, severity, and clinical features of acute and chronic pancreatitis in patients with systemic lupus erythematosus. Rheumatology International, 36(10):1413-1419.
Publisher | Google Scholor - Rim, D., Kaye, A., Choi, C., & Ahlawat, S. (2021). Inpatient outcomes of acute pancreatitis among patients with systemic lupus erythematosus: A nationwide analysis. Cureus, 13(7).
Publisher | Google Scholor - Makol, A., & Petri, M. (2010). Pancreatitis in systemic lupus erythematosus: Frequency and associated factors — A review of the Hopkins Lupus Cohort. The Journal of Rheumatology, 37(2):341-345.
Publisher | Google Scholor - Derk, C. T., & DeHoratius, R. J. (2004). Systemic lupus erythematosus and acute pancreatitis: a case series. Clinical Rheumatology, 23(2):147-151.
Publisher | Google Scholor - Narváez, J. (2020). Lupus eritematoso sistémico 2020. Medicina Clínica, 155(11):494-501.
Publisher | Google Scholor - Monteagudo, D. E., Kokuina, E., Peña, Y., Porben, S. S., & Hernández, D. M. (2020). Sobre la capacidad discriminativa de diferentes autoanticuerpos en el diagnóstico del Lupus Eritematoso Sistémico. DOAJ (Directory of Open Access Journals).
Publisher | Google Scholor - Fanouriakis, A., Kostopoulou, M., Alunno, A., Aringer, M., Bajema, I., et al. (2019). 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Annals of the Rheumatic Diseases, 78(6):736-745.
Publisher | Google Scholor























