

Case Report
A Systematic Review of the Effectiveness of Contraceptive Mobile Apps in Preventing Unintended Pregnancies in Women of Reproductive Age Group in Comparison to Standard Care or Alternative Digital Interventions
- Quagy Siamalambwa 1
- Stylianos Sergios Chatziioannou 2,3*
- Varvara Papasideri 4
- Georgios Salvanos 3
- Chibesa Chalwe 5
1Department of Obstetrics and Gynaecology, Choma General Hospital, Choma, Zambia.
2School of Medicine, European University of Cyprus, Nicosia, Cyprus.
3First Department of Obstetrics and Gynecology, Maternity Hospital, Elena Venizelou, Athens, Greece.
4 School of Humanities, Social and Education Sciences, Department of Psychology, European University of Cyprus, Nicosia, Cyprus.
5Department of Obstetrics and Gynaecology, Mansa General Hospital, Mansa, Zambia.
*Corresponding Author: Stylianos Sergios Chatziioannou, School of Medicine, European University of Cyprus, Nicosia, Cyprus.
Citation: Siamalambwa Q, Stylianos S. Chatziioannou, Papasideri V, Salvanos G., Chalwe C. (2025). A Systematic Review of the Effectiveness of Contraceptive Mobile Apps in Preventing Unintended Pregnancies in Women of Reproductive Age Group in Comparison to Standard Care or Alternative Digital Interventions, Journal of BioMed Research and Reports, BioRes Scientia Publishers. 8(4):1-17. DOI: 10.59657/2837-4681.brs.25.200
Copyright: © 2025 Stylianos Sergios Chatziioannou, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 30, 2025 | Accepted: September 11, 2025 | Published: September 20, 2025
Abstract
Background: Mobile contraceptive applications are innovative tools for improving reproductive health, particularly in resource-limited settings. These apps aim to enhance contraceptive knowledge, adherence, and use, potentially reducing unintended pregnancies. However, their effectiveness varies, with systemic barriers often limiting outcomes, especially in low- and middle-income countries (LICs).
Objective: This review evaluates the effectiveness of contraceptive mobile applications in preventing unintended pregnancies among women aged 15–49. It also compares their performance with standard care and other digital interventions, highlighting associated challenges and future research needs.
Methodology: A systematic search was conducted in PubMed, Embase, the Cochrane Library, and Scopus, adhering to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Eight studies (2013–2023), including six randomized controlled trials (RCTs) and two observational studies, were reviewed. These studies assessed the impact of mobile contraceptive applications on knowledge, adherence, and use across diverse populations and settings, with a focus on LICs and high-income countries (HICs).
Results: Fertility-awareness-based apps, such as "Natural Cycles," showed effectiveness comparable to traditional methods under perfect use, with a Pearl Index of 1.0. Typical-use effectiveness was lower, with Pearl Indices of 6.9 to 7.0, indicating adherence challenges. Apps improved contraceptive knowledge and acceptability, but their impact on usage and unintended pregnancy rates was inconsistent. Barriers included digital literacy gaps, engagement variability, and privacy concerns.
Conclusion: Contraceptive mobile applications hold promise for advancing reproductive health but require improved user engagement, integration with standard care, and solutions to systemic barriers. Future research should focus on enhancing app functionality, long-term impacts, and accessibility to maximize their potential in diverse populations.
Keywords: contraceptive mobile applications; unintended pregnancies; mhealth interventions; reproductive health; digital health equity
Introduction
Unintended pregnancies continue to pose a significant challenge to public health, affecting women of reproductive age worldwide. According to the World Health Organisation (WHO), approximately 121 million unintended pregnancies occur annually, with the highest rates observed in low- and middle-income countries (LMICs) (World Health Organisation, 2021). These pregnancies can lead to adverse health outcomes, including maternal mortality, unsafe abortions, and compromised economic and social well-being for women and their families (UNFPA, 2022). Despite the availability of effective contraceptive methods, barriers such as limited access to healthcare, cultural norms, and gaps in education prevent many women from using these resources effectively (Winner et al., 2012). In this context, digital health solutions, particularly mobile applications (apps), have emerged as innovative tools to address these barriers and improve family planning outcomes (Free et al., 2013).
The rapid advancement of mobile technology has revolutionised healthcare delivery across various domains. Mobile health (mHealth) applications offer user-friendly, accessible, and cost-effective platforms for managing diverse health needs (Hollander and Carr, 2020). In reproductive health, these apps provide features such as menstrual cycle tracking, fertility predictions, contraceptive reminders, and educational resources tailored to the user's preferences and needs (Duane et al., 2016). By empowering women with knowledge and tools to make informed decisions about their reproductive health, mobile contraceptive apps have the potential to bridge existing gaps in traditional healthcare systems (Mangone, Lebrun, & Muessig, 2016). This potential is particularly relevant in LMICs, where resource constraints often limit access to standard contraceptive counselling and services (World Health Organisation, 2016).
The role of digital interventions in reproductive health is increasingly recognized. The WHO has emphasised the potential of mHealth technologies to address critical reproductive health challenges, particularly in underserved populations (World Health Organisation, 2021). These interventions align with global public health priorities, such as the Sustainable Development Goals (SDGs), which aim to ensure universal access to sexual and reproductive health services by 2030 (United Nations, 2015) Mobile apps offer scalable and adaptable solutions, making them an attractive option for governments, non-governmental organisations (NGOs), and healthcare providers seeking to improve contraceptive use and reduce unintended pregnancies (Free et al., 2013).
A variety of contraceptive mobile apps are currently available, catering to diverse user needs and preferences. Fertility-awareness-based apps, such as "Natural Cycles" and "Clue," help users track their menstrual cycles and identify fertile windows (Berglund Scherwitzl et al., 2017a). These apps rely on algorithms that analyse user-inputted data, such as basal body temperature and menstrual cycle length, to predict ovulation and fertility patterns (Duane et al., 2016). By providing personalised insights, these apps empower women to manage their reproductive health autonomously. However, their effectiveness varies depending on user adherence and the accuracy of the data entered (Guse et al., 2012). Studies have shown that while fertility-awareness-based apps can be as effective as some traditional contraceptive methods under perfect use, their typical-use failure rates are higher due to inconsistent adherence (Berglund Scherwitzl et al., 2017a).
Beyond fertility-awareness-based apps, other mHealth tools aim to enhance contraceptive access and adherence through innovative features. For instance, some apps provide reminders for contraceptive pill use, schedule alerts for follow-up visits, and access to educational content about different contraceptive methods (Mangone, Lebrun and Muessig, 2016). These features are particularly valuable for women who face challenges accessing traditional healthcare services due to cost, distance, or social stigma (Guse et al., 2012). By offering discreet and convenient access to reproductive health resources, mobile apps address many of the barriers that hinder contraceptive use (Stifani et al., 2021).
The potential of mobile contraceptive apps is not limited to high-income settings. In LMICs, where healthcare infrastructure is often inadequate, these tools can play a transformative role in expanding access to family planning services (World Health Organisation, 2016). Mobile phone penetration rates are rapidly increasing in many LMICs, providing an opportunity to leverage digital technology for public health interventions (Comfort et al., 2022). For example, mobile apps can serve as a cost-effective alternative to in-person counselling, delivering the accurate and culturally appropriate information to users in remote or underserved areas (Raymond et al., 2019). Moreover, the anonymity and privacy offered by apps make them particularly appealing to women in conservative societies, where discussing reproductive health openly may be taboo (Mangone, Lebrun and Muessig, 2016).
Despite their potential, the effectiveness of contraceptive mobile apps remains a subject of debate. While some studies highlight their ability to improve contraceptive knowledge and adherence (Guse et al., 2012; Free et al., 2013), others question their impact on reducing unintended pregnancies. Research suggests that the success of these apps depends on several factors, including user engagement, digital literacy, and the integration of app-based interventions with existing healthcare systems (Winner et al., 2012). For instance, a systematic literature search and review by Guse et al. (2012) found that while mobile apps improved contraceptive knowledge among young women, their impact on unintended pregnancy rates was inconsistent. Similarly, Duane et al. (2016) noted that fertility-awareness-based apps are susceptible to user error, limiting their reliability compared to long-acting reversible contraceptives (LARCs), which do not depend on user adherence (American College of Obstetricians and Gynaecologists, 2021).
The importance of addressing these limitations is underscored by the growing reliance on digital health interventions in global reproductive health strategies (United Nations, 2015). The COVID-19 pandemic has further highlighted the need for accessible and scalable healthcare solutions, as traditional services faced disruptions worldwide (Stifani et al., 2021). During this period, telemedicine and mobile apps played a critical role in sustaining contraceptive access, demonstrating their adaptability and resilience in challenging circumstances (Raymond et al., 2019). For instance, the TelAbortion project showed how telehealth platforms could provide safe and effective reproductive healthcare remotely, offering insights into the potential synergies between mobile apps and professional healthcare services (Comfort et al., 2022).
While contraceptive mobile apps offer several advantages, their limitations must be acknowledged to maximise their effectiveness. One significant challenge is user engagement. High dropout rates have been reported for many apps, often due to dissatisfaction with app design, perceived complexity, or lack of perceived benefits (Scherwitzl et al., 2016). For example, a study by Scherwitzl et al. (2016) reported a discontinuation rate of 54.6% among users of the Natural Cycles app over 12 months, with 24% citing dissatisfaction as the reason for discontinuation. Addressing these issues requires a focus on user-centered design, incorporating features such as gamification, personalised feedback, and interactive support to enhance engagement and retention (Hollander & Carr, 2020).
Privacy and security concerns also pose challenges for contraceptive mobile apps. As these tools collect sensitive personal data, such as menstrual cycle information and sexual activity, ensuring robust data protection measures is essential (American College of Obstetricians and Gynaecologists, 2021). Fear of data breaches or misuse of personal information may deter users from fully engaging with these platforms (Gomez et al., 2021). Developers must prioritize transparent data policies, secure authentication methods, and compliance with international regulations, such as the General Data Protection Regulation (GDPR), to build user trust (Guse et al., 2012).
Digital literacy and access disparities further limit the reach of contraceptive mobile apps, particularly in LMICs (World Health Organisation, 2016). While mobile phone penetration rates are increasing, significant gaps remain in smartphone ownership and internet connectivity, particularly among low-income and rural populations (Comfort et al., 2022). Addressing these inequities requires targeted interventions, such as subsidized mobile devices, offline app functionality, and digital literacy programs (Mangone, Lebrun, & Muessig, 2016). Partnerships with local governments and NGOs can help bridge these gaps, ensuring that digital health solutions are accessible to all (Kruse et al., 2017).
The integration of mobile contraceptive apps with standard care and telehealth services offers a promising pathway to enhance their impact (Hollander & Carr, 2020). By combining the convenience and accessibility of apps with the expertise of healthcare professionals, integrated models can address the limitations of standalone digital interventions (Raymond et al., 2019). For instance, apps can serve as a first point of contact, providing users with basic information and guiding them to telehealth consultations or in-person services for more comprehensive care (Comfort et al., 2022). Studies have shown that hybrid models combining digital and professional support improve user outcomes and satisfaction, highlighting the potential of such approaches in reproductive healthcare (Free et al., 2013).
Future research should explore the long-term impacts of mobile contraceptive applications on reproductive health outcomes. Longitudinal studies are needed to assess how sustained engagement with these tools influences contraceptive use, unintended pregnancy rates, and broader health metrics (Guse et al., 2012). Comparative studies examining the integration of apps with telehealth and standard care can provide valuable insights into best practices for optimizing digital interventions (Hollander & Carr, 2020). Expanding research efforts to include qualitative studies will also help illuminate user experiences and identify areas for improvement (Stifani et al., 2021).
Mobile contraceptive applications represent a promising innovation in reproductive healthcare. They offer accessible, cost-effective, and user-centred solutions for family planning, particularly in resource-constrained settings (World Health Organisation, 2016). However, their effectiveness depends on addressing adherence challenges, integrating with professional care, and overcoming systemic barriers such as digital inequities (United Nations, 2015). These tools can play a transformative role in improving global reproductive health outcomes by leveraging technology and fostering collaborations between developers, healthcare providers, and policymakers.
The main objective of this literature review is to evaluate the effectiveness of mobile applications in supporting contraceptive use and preventing unintended pregnancies among women of reproductive age (15-49 years).
Methods
This study employed a systematic literature search and review methodology to evaluate the effectiveness of contraceptive mobile applications in preventing unintended pregnancies. The methodology adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Literature Search and Reviews and Meta-Analyses (PRISMA) framework, ensuring the review was conducted with transparency, reproducibility, and methodological rigour. This approach facilitated a robust assessment of the available evidence and minimised potential biases throughout the research process.
The study design incorporated a series of meticulously planned steps to achieve its objectives:
Research Question Formulation
The primary research question was designed to determine whether contraceptive mobile apps are more effective in reducing unintended pregnancies compared to standard care or alternative digital interventions. Secondary objectives included evaluating the usability, adherence, and overall user satisfaction with these applications.
Comprehensive Literature Search
A comprehensive and structured search strategy was developed to identify relevant studies using major electronic databases, including PubMed, Embase, the Cochrane Library, and Google Scholar. While Scopus was initially planned, it was excluded due to access challenges, and Google Scholar was included instead, despite not being part of the original plan. Boolean operators "AND" and "OR" were used to refine the search queries, incorporating key terms such as “contraceptive mobile apps,” “mHealth,” “unintended pregnancies,” “adherence,” “usability,” and “effectiveness.” To ensure thoroughness, supplementary searches included reviewing bibliographies of relevant articles and obtaining recommendations from domain experts. This approach aimed to maximise the scope and comprehensiveness of the search process.
Screening and Selection
A comprehensive two-phase screening process was meticulously conducted to ensure the inclusion of relevant studies. During the initial phase, titles and abstracts of identified articles were thoroughly reviewed to determine their potential relevance to the research objectives. This step served as a preliminary filter, narrowing down the pool of studies by excluding those unrelated to the topic. The second phase involved a more detailed examination, where full-text articles were assessed against a set of predefined inclusion and exclusion criteria. Studies qualified for inclusion if they specifically evaluated mobile applications aimed at preventing unintended pregnancies. Additionally, only studies reporting outcomes directly relevant to the research question were considered. To maintain temporal relevance, the analysis was restricted to studies published within the specified timeframe, from 1 January 2013 to 31 December 2023. This rigorous approach ensured that only high-quality and pertinent studies were included in the final analysis.
Data Collection and Quality Assessment
To ensure consistency, accuracy, and reliability in the review process, data were systematically extracted from all included studies using a standardised data extraction form. This approach facilitated uniformity in capturing relevant details, minimizing errors, and promoting transparency in the synthesis of findings. Alongside data extraction, quality assessment tools were employed to evaluate the methodological rigour of the included studies. For randomised controlled trials, the Cochrane Risk of Bias tool (ROB-1) was utilised, providing a structured framework to assess potential biases in study design and execution. Observational studies were assessed using the Newcastle-Ottawa Scale, a widely recognised tool for evaluating study quality based on selection, comparability, and outcomes. The combined use of these tools ensured a robust evaluation of the evidence base, enhancing the validity, reliability, and interpretability of the findings, and supporting evidence-based conclusions.
Synthesis of Findings
A narrative synthesis was employed to summarise the key findings across all the included studies, providing a comprehensive overview of the available evidence. This approach was chosen because it was not feasible to apply quantitative methods, such as meta-analysis, which would have aggregated data and computed overall effect sizes. Despite initial intentions to use meta-analytic techniques, the variability in study designs, populations, and outcome measures across the included studies made such statistical pooling impractical. Instead, the narrative synthesis allowed for a descriptive exploration of patterns, themes, and relationships within the data, offering valuable insights into the findings while acknowledging the methodological constraints.
This systematic literature search and review design provided a comprehensive evaluation of the effectiveness, usability, and adherence of contraceptive mobile apps, offering valuable insights into their role in reproductive health.
Data Sources
Comprehensive literature searches were conducted across multiple databases, including PubMed, Embase, Cochrane Library, and Google Scholar. Although Google Scholar was not originally cited in the project proposal, it was included in place of the challenge-laden Scopus to ensure a more exhaustive retrieval of relevant studies. The search terms were strategically designed to include combinations of keywords such as "contraceptive mobile apps," "unintended pregnancies," "mHealth," "adherence," "usability," and "effectiveness." These terms were carefully chosen to capture a wide range of studies focusing on mobile health interventions to prevent unintended pregnancies. The inclusion of multiple databases and diverse search terms ensured that the search process was thorough, comprehensive, and inclusive of relevant publications, maximising the likelihood of identifying all pertinent research articles.
Search Strategy
The search strategy employed Boolean operators "AND" and "OR" to systematically refine and broaden the search results. The formulated search query was structured as ["contraceptive mobile applications" OR "mHealth"] AND "unintended pregnancies" AND ["adherence" OR "usability"] AND "effectiveness," targeting a comprehensive range of relevant studies. Additionally, supplementary searches were conducted, which included examining the bibliographies of retrieved articles for potential sources and seeking recommendations from domain experts to ensure a thorough identification of eligible studies.
The review specifically focused on research published between January 1, 2013, and December 31, 2023, to capture the most recent advancements and findings. This approach aimed to encompass studies addressing the effectiveness, usability, and adherence of mobile health interventions for preventing unintended pregnancies, ensuring relevance and reliability in the data collected for analysis.
Inclusion and Exclusion Criteria
| Inclusion Criteria | Exclusion Criteria |
| Research published in the English language. | Research not related to contraceptive mobile apps. |
| Research evaluating the effectiveness of contraceptive mobile apps in preventing unintended pregnancies in women aged 15 to 49 years of age. | Research without clear outcomes related to unintended pregnancies. |
| Randomised controlled trials (RCTs), cohort studies, and observational studies. | Reviews, editorials, and opinion pieces. |
| Publications before January 2013 and after 31 December 2023 |
Data Extraction and Quality Assessment
Data extraction was conducted systematically using a standardised form (see appendix 1), designed to capture essential details from each included study. The form recorded key information such as the study design, study population characteristics, intervention details, and outcomes reported. This consistent approach ensured thoroughness and minimised variability in the data collection process, enabling a reliable comparison across the included studies.
Rigorous assessment tools were employed to evaluate the methodological quality of the studies. The Cochrane Risk of Bias (ROB 1) tool was used for randomised controlled trials. This tool provided a structured framework for identifying potential biases in study design, implementation, and reporting, ensuring a robust evaluation of trial quality. For observational studies, the Newcastle-Ottawa Scale (NOS) was applied. The NOS evaluates methodological rigour by assessing three primary domains: the selection of study groups, the comparability of groups, and the ascertainment of outcomes of interest.
Data Synthesis and Analysis
A narrative synthesis was conducted to provide a detailed and comprehensive overview of the main findings from the research. While the initial plan involved conducting a meta-analysis to assess and summarise the overall effectiveness of the interventions quantitatively, this approach was ultimately deemed unfeasible due to various factors. These included issues such as insufficient data consistency across studies, variability in intervention methodologies, and limited availability of comparable outcome measures, which collectively hindered quantitative integration.
Outcomes
The primary outcome of the study was to evaluate the effectiveness of mobile applications in preventing unintended pregnancies among women in the reproductive age group. The secondary outcomes focused on a comprehensive evaluation of the usability and user experience related to these mobile applications. This included analysing how effectively users interacted with the apps and their overall satisfaction levels. Additionally, we aimed to assess adherence to the app's functionalities and features, all in the context of their primary goal: to successfully prevent unintended pregnancies. The study aimed to explore how well these apps were designed, their accessibility, and their overall impact on behaviour change in the target population.
Results
This systematic literature search and review cover studies published between January 2013 and December 2023, focusing on peer-reviewed literature to ensure the inclusion of high-quality, evidence-based materials. The search strategy was comprehensive, including diverse study designs to provide a nuanced understanding of the effectiveness of contraceptive mobile applications in reducing unintended pregnancies among women of reproductive age.
A total of eight studies met the inclusion criteria, consisting of six randomised controlled trials (RCTs) and two observational studies. RCTs offered strong evidence of the interventions’ effectiveness under controlled settings, while observational studies provided insights into real-world use and difficulties. The included studies assessed mobile applications designed for contraceptive use, comparing their results with standard care practices or alternative digital options. Follow-up durations ranged from 3 to 12 months, allowing evaluation of both short-term and medium-term effectiveness.
The sample sizes across the studies varied considerably, ranging from 221 to 22,785 participants. This broad span reflects the diverse populations and settings included in the review. Geographically, five of the eight studies were carried out in low-income countries (LICs), emphasising the increasing importance of mobile health interventions in resource-limited environments. Conversely, only three studies were from high-income countries (HIC), indicating a gap in research on mobile contraceptive applications in these areas.
Study selection followed a thorough screening process, guided by the Preferred Reporting Items for Systematic literature search and reviews and Meta-Analyses (PRISMA) guidelines, as shown in Figure 1. This ensured that only relevant and methodologically sound studies were included in the review.
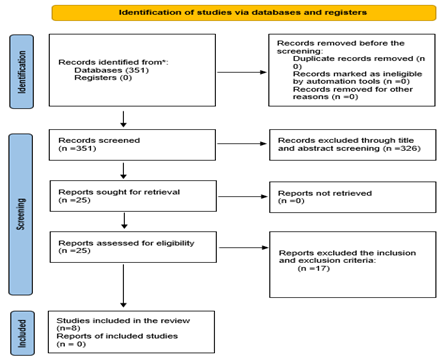
Figure 1: PRISMA flow diagram adapted from (Page et al., 2021).
Study Characteristics
Table: 1
| Author | Country | Population Characteristics | Study Design | Sample Size | Duration | App Evaluated | Key Features |
| (Berglund Scherwitzl et al., 2016) | Sweden | HIC | Observational | 1233 | 7 months | Natural Cycle App | Tracks menstrual cycle, ovulation, and fertility. |
| (McCarthy et al., 2018) | Tajikistan | LIC | RCT | 573 | 4 months | Messaging App | Reminders and education content |
| (Berglund Scherwitzl et al., 2017) | 37 different countries with 79% from Sweden | Majority HIC | Observational | 22,785 | 12 months | Natural Cycle App | Menstrual cycle and basal body temperature tracking |
| (McCarthy et al., 2020) | Bolivia | LIC | RCT | 640 | 4 months | Messaging App | Educational content to influence behaviour |
| (Smith et al., 2015) | Cambodia | LIC | RCT | 500 | 12 months | Messaging App | Educational content on contraceptive method and followed by reminders on those who chose short methods |
| (Hebert et al., 2018) | United States of America | HIC | RCT | 221 | 12 months | miPlan (counselling) App | Educational Content |
| (Reiss et al., 2019) | Bangladeshi | LIC | RCT | 969 | 4 months | Messaging App | Educational content on LARC fears |
| (McCarthy et al., 2019) | Palestine | LIC | RCT | 582 | 4 months | Messaging App | Education content |
The studies selected for the review displayed the following summaries of characteristics.
Low-income Countries
McCarthy et al., 2018: A randomised controlled trial was conducted to assess the effectiveness of a mobile phone app-based intervention aimed at increasing the acceptability of effective contraception among young people in Tajikistan. The study involved 573 participants aged 16 to 24, who were randomly assigned to either an intervention group, which received tailored contraceptive education via app-based instant messaging, or a control group, which was provided with standard information. The main outcome measured was the acceptability of at least one effective contraceptive method four months after the start of the intervention.
Results showed that 66% of participants in the intervention group found at least one method acceptable, compared to 64% in the control group. This small difference was not statistically significant (adjusted odds ratio 1.21, 95% confidence interval 0.80–1.83, p = 0.36). However, when data from both groups were combined, there was a notable increase in overall acceptability rates, which rose markedly from 2% at baseline to 65% at follow-up (p less than 0.001). These findings indicate that the app content, which included accurate and engaging information about contraception, may have positively influenced participants' attitudes and willingness to consider effective contraceptive options. Although the study did not show significant differences between the intervention and control groups, it highlights the wider potential of mobile health interventions to enhance knowledge and acceptance of contraception.
McCarthy et al., 2020: A randomised controlled trial was conducted to evaluate the effectiveness of a mobile phone app-based intervention designed to increase the acceptability and use of effective contraception among young women in Bolivia. The study recruited 640 women aged 16 to 24 who had an unmet need for contraception. Participants were randomly allocated to one of two groups: an intervention group that received tailored contraceptive education via app-based instant messaging, or a control group that received standard information. The primary outcomes measured after four months included the use and acceptability of at least one effective contraceptive method.
Results indicated that 37% of participants in the intervention group reported using effective contraception, compared to 33% in the control group. However, this difference was not statistically significant (adjusted odds ratio [OR] 1.19, 95% confidence interval [CI] 0.80–1.77; P = .40). Regarding acceptability, 72% of the intervention group found at least one method acceptable, compared to 63% in the control group, with a borderline significant effect (adjusted OR 1.49, 95% CI 0.98–2.28; P = .06). Secondary outcomes, such as service uptake, unintended pregnancies, and abortion rates, showed no significant differences between the two groups. The study faced challenges, including under-recruitment and a low intervention dose received by participants, which limited the ability to make definitive conclusions. Despite these limitations, the findings highlight the potential of mobile health interventions to improve contraceptive acceptability among young women in Bolivia.
Smith et al., 2015: A randomised controlled trial conducted in Cambodia, as part of the Mobile Technology for Improved Family Planning (MOTIF) study, evaluated a mobile phone-based intervention designed to promote post-abortion contraceptive use. The study included 500 women who had received safe abortion services at four Marie Stopes International clinics. Participants were randomly allocated to one of two groups: an intervention group that received six interactive voice messages with optional counsellor support, or a control group that received standard post-abortion care. The primary aim was to assess how effective the intervention was in improving contraceptive uptake. At four months post-abortion, 64% of women in the intervention group reported using effective contraception, compared to 46% in the control group (relative risk [RR]: 1.39; 95% confidence interval [CI]: 1.17–1.66). However, by 12 months, the difference between the groups was no longer significant, with contraceptive use reported at 50% in the intervention group versus 43% in the control group (RR: 1.16; 95% CI: 0.92–1.47). Notably, the intervention group demonstrated a higher uptake of long-acting contraceptive methods at both follow-up points. There were no notable differences between the two groups in repeat pregnancies or abortion rates at either four or 12-months. These results indicate that mobile interventions can improve short-term contraceptive use, especially for long-acting methods, when incorporated into post-abortion care.
McCarthy et al., 2019: A randomised controlled trial conducted in Palestine evaluated the effectiveness of a mobile phone text message intervention aimed at increasing the acceptability of effective contraception among young women. The study enrolled 578 women aged 18 to 24 who were not currently using any effective contraceptive methods. Participants were randomly allocated to one of two groups: the intervention group, which received up to three tailored text messages daily for 120 days, or the control group, which received neutral messages centred on trial participation.
After four months, 31% of participants in the intervention group reported finding at least one effective contraceptive method acceptable, compared to only 17% in the control group. This represented a significant difference, with an adjusted odds ratio of 2.34 (95% confidence interval 1.48–3.68; p less than 0.001). The intervention group also exhibited higher knowledge scores about contraception and greater acceptability of specific methods, such as intrauterine devices (IUDs), contraceptive injections, implants, and patches. However, the study found no significant differences between the intervention and control groups in actual use of effective contraception after four months, nor in secondary outcomes like service uptake, unintended pregnancies, or induced abortions. These findings demonstrate the potential of tailored text messaging interventions to enhance contraceptive acceptability and knowledge but highlight the need for further strategies to turn these improvements into actual behavioural change.
Reis et al., 2019: A randomised controlled trial conducted in Bangladesh assessed the impact of automated interactive voice messages (IVMs) on contraceptive use among women following menstrual regulation (MR). The study involved 969 participants recruited from 41 clinics, who were randomly allocated to either an intervention or a control group. Women in the intervention group received 11 IVMs over four months promoting long-acting reversible contraceptives (LARCs), while those in the control group received no messages. The primary outcome was LARC use at the four-month follow-up, with secondary outcomes examining experiences of intimate partner violence (IPV). At the end of four months, 12% of participants in the intervention group reported using LARCs, compared to 15% in the control group. This difference was not statistically significant (adjusted odds ratio [aOR] 0.95; 95% confidence interval [CI] 0.49–1.83; P = .22). Interestingly, reports of physical IPV were notably higher among participants in the intervention group (11%) compared to the control group (7%), with a significant adjusted odds ratio of 1.97 (95% CI 1.12–3.46; P = .03). Open-ended questions revealed no IPV incidents, highlighting the importance of direct questioning for accurate reporting of such experiences. The study’s findings show that while the mHealth intervention did not lead to higher LARC uptake, it was unexpectedly linked to an increase in self-reported IPV.
High-income Countries
Scherwitzl et al., 2016: A retrospective analysis was conducted to evaluate the contraceptive effectiveness of the Natural Cycles mobile app, a fertility awareness-based method that predicts fertile days by analysing basal body temperature and menstrual cycle data. The study involved data from 4,054 women using the app for contraception, amounting to 2,085 woman-years of usage. The results revealed a typical-use Pearl Index of 7.0, indicating seven unintended pregnancies per 100 woman-years. For perfect use, where users strictly adhered to the app’s advice, the Pearl Index was significantly lower at 1.0, representing one unintended pregnancy per 100 woman-years. The study also pointed out challenges with user engagement, reporting a discontinuation rate of 54.6% over 12 months. Among those who stopped using the app, 24.0% cited dissatisfaction with the method as their reason for discontinuing.
Scherwitzl et al., 2017: A prospective observational study was carried out to assess the contraceptive effectiveness of the Natural Cycles mobile app, a fertility awareness-based method that relies on basal body temperature and menstrual cycle data to accurately predict fertile days. The study examined a substantial dataset from 22,785 users, amounting to a total of 18,548 woman-years of usage. The results showed a typical-use Pearl Index of 6.9, meaning around seven unintended pregnancies occur per 100 woman-years of use. For users who followed the app's advice exactly, the Pearl Index dropped to 1.0, corresponding to one unintended pregnancy per 100 woman-years.
Hebert et al., 2018: A randomised controlled trial was conducted to evaluate the impact of the miPlan mobile application on contraceptive counselling and decision-making. The study included 207 African American and Latina women aged 15 to 29 who were attending four family planning clinics in a large Midwestern city. Participants were randomly assigned to either an intervention group, which used the miPlan app prior to their clinic visit, or a control group, which received standard contraceptive counselling without app use. The findings showed that immediately after using the app, participants in the intervention group demonstrated increased knowledge about contraceptive effectiveness and expressed a greater interest in learning about contraceptive implants compared to the control group. However, there was no significant difference observed between the two groups in the immediate uptake of long-acting reversible contraception (LARC) following their clinic visits. At the three-month follow-up, app users demonstrated significantly greater knowledge of intrauterine device (IUD) effectiveness compared to controls (52.3% vs. 30.8%, p = .001). Despite this increase in knowledge, there was no significant difference between the groups in actual LARC usage over the study period.
Quality Analysis Studies Selected
The quality of the chosen studies was evaluated by examining their strengths, weaknesses, and biases. The Cochrane Risk of Bias tool (ROB-1) was used for randomised controlled trials (figure 2), while the Newcastle-Ottawa Scale was applied to assess observational studies (figure 3).

Figure 2: Risk of bias assessment with Cochrane ROB-1 tool for RCTs

Figure 3: Newcastle-Ottawa scale for ROB assessment of non-randomised studies
Effectiveness of Contraceptive Applications
Reduction in Unintended Pregnancies
Mobile health (mHealth) interventions have demonstrated mixed results in reducing unintended pregnancies across various contexts. In Tajikistan, McCarthy et al. (2018) reported no statistically significant difference in the acceptability of effective contraception between intervention and control groups. However, the study did highlight a remarkable increase in overall acceptability rates within the intervention group, which rose dramatically from 2% at baseline to 65% by the end of the study period. Similarly, in Bolivia, McCarthy et al. (2020) observed no statistically significant impact on the actual use of effective contraception. Despite this, acceptability among participants in the intervention group increased, with 72% of participants finding at least one method acceptable compared to 63% in the control group, suggesting improved awareness or perceived value of contraception facilitated by the intervention.
In Cambodia, Smith et al. (2015) found that mobile health interventions were effective in increasing contraceptive use shortly after an abortion, with usage rates at four months post-intervention rising significantly to 64% in the intervention group compared to 46% in the control group. However, this effect diminished over time, with no significant differences observed at the 12-month mark. In Bangladesh, Reis et al. (2019) reported no improvement in the uptake of long-acting reversible contraceptives (LARCs) despite the use of mobile intervention strategies. Additionally, the study raised concerns about unintended consequences, such as an increase in self-reported incidents of intimate partner violence (IPV), underscoring the potential social risks and challenges associated with implementing these types of interventions in certain cultural and social contexts.
In high-income countries, digital contraceptive tools like the Natural Cycles app have been assessed. Scherwitzl et al. (2016, 2017) reported a Pearl Index of 1.0 for perfect use, indicating effectiveness comparable to traditional methods like oral contraceptives. However, for typical use, the index ranged between 6.9 and 7.0, revealing significant challenges with adherence.
Adherence and Usability
Adherence and usability were recurring and critical themes across the studies reviewed. Tailored messaging and interactive features embedded in mobile health (mHealth) tools were shown to improve users’ knowledge and satisfaction levels. For instance, McCarthy et al. (2018, 2020) reported increased contraceptive acceptability in Tajikistan and Bolivia due to accurate and accessible education delivered through mobile applications. In Palestine, McCarthy et al. (2019) demonstrated significant improvements in contraceptive acceptability and knowledge scores (adjusted OR 2.34), reflecting positive attitudes fostered by mobile text-based interventions.
Scherwitzl et al. (2016, 2017) further highlighted that user adherence played a pivotal role in determining effectiveness, with typical-use outcomes significantly lagging behind those observed under perfect-use conditions. Despite the usability advantages offered by mHealth tools, such as personalised feedback, accessibility, and convenience, high dropout rates—like the 54.6% reported by Scherwitzl et al. (2016)—exposed significant engagement challenges that hindered long-term adherence.
Comparative Performance
Compared to traditional contraceptive methods, mobile health (mHealth) interventions demonstrated varying levels of performance across different studies and contexts. Smith et al. (2015) found that mobile-based counselling interventions significantly increased short-term contraceptive use among post-abortion patients, although they lacked the sustained efficacy seen with long-acting reversible contraceptives (LARCs). Similarly, Reis et al. (2019) observed no significant improvement in LARC uptake through the use of voice message interventions, highlighting the superior reliability of non-user-dependent contraceptive methods, which are less influenced by individual adherence.
Fertility-awareness-based applications, such as those evaluated by Scherwitzl et al. (2016, 2017), achieved outcomes comparable to oral contraceptives under perfect-use conditions. However, these tools proved less effective in real-world scenarios due to challenges with consistent and accurate user adherence. Despite these limitations, mHealth tools offer several advantages, including enhanced privacy, improved accessibility, and cost-effectiveness, making them particularly appealing to specific populations seeking convenient and non-invasive options.
However, standalone mHealth apps are often outperformed by telemedicine platforms, which integrate digital tools with direct healthcare provider involvement. This integration, as seen in Smith et al. (2015), ensures a more comprehensive approach to care, enhancing the effectiveness of interventions.
Key Features of the Contraceptive Mobile Applications
Personalization: Contraceptive mobile applications offer highly personalised experiences designed to meet the unique reproductive health needs of individual users. These tools provide customised insights by utilising user-specific data, such as basal body temperature and menstrual cycle patterns, to predict fertile days, as seen in apps like Natural Cycles. Such features enable users to make informed decisions about their contraceptive methods. However, the overall effectiveness of these apps is heavily dependent on user adherence, with typical-use Pearl Indices being significantly higher than those for perfect use (e.g., 6.9 compared to 1.0; Scherwitzl et al., 2016, 2017), reflecting challenges with consistent use.
Tailored messaging has also proven effective in improving contraceptive acceptability. For example, McCarthy et al. (2018, 2020) highlighted how personalised messages delivered through mobile apps in countries such as Tajikistan and Bolivia significantly increased users’ knowledge and acceptability of contraceptive methods. However, these interventions often did not lead to corresponding increases in actual usage, underscoring the importance of addressing additional factors influencing user behaviour and adherence.
Accessibility: Mobile applications play a crucial role in bridging gaps in contraceptive access, particularly in low- and middle-income countries (LMICs), where traditional healthcare services may be limited or difficult to access. In Cambodia, Smith et al. (2015) demonstrated that mobile interventions significantly increased contraceptive uptake among post-abortion patients, with 64% of participants in the intervention group reporting contraceptive use compared to 46% in the control group. These applications help eliminate barriers such as the distance to healthcare facilities by offering users greater autonomy and privacy in managing their reproductive health needs. However, as noted by Reis et al. (2019) in Bangladesh, critical infrastructure gaps, including unreliable internet connectivity and limited smartphone access, can restrict the reach and effectiveness of these interventions, especially in rural areas.
Community and Support: Community and support features significantly enhanced the utility of mobile applications by helping to sustain user engagement over time. Smith et al. (2015) demonstrated the effectiveness of integrating counsellor support with voice message interventions, which successfully boosted the uptake of long-acting reversible contraception (LARC) among participants. Similarly, peer forums and structured support systems can play a vital role in addressing issues such as user dissatisfaction and high dropout rates, as observed in Scherwitzl et al. (2016, 2017). Adding interactive elements, such as gamified content, personalised feedback, or real-time discussion forums, could further improve outcomes by fostering user motivation, encouraging active participation, and promoting shared learning experiences among users.
Discussion
The findings from this review highlight the considerable potential of mobile contraceptive applications in enhancing access to reproductive health information and services, especially in settings with limited resources. These digital tools can bridge gaps in healthcare access by providing crucial information and supporting informed decision-making. However, their effectiveness in reducing unintended pregnancies remains inconsistent and is influenced by several key factors. These include user adherence to the applications, equitable access to the required technology, and the extent to which these tools are integrated into broader healthcare systems.
Effectiveness in Low-Income Countries
In low-income countries (LICs), mobile apps were shown to increase contraceptive acceptability but demonstrated limited impact on actual usage. For instance, McCarthy et al. (2018, 2020) observed no significant differences in contraceptive use between intervention and control groups in Tajikistan and Bolivia, though acceptability rates improved substantially. These findings underscore the importance of tailored educational content delivered via mobile platforms in influencing attitudes toward contraception. Smith et al. (2015) found that mobile interventions increased contraceptive uptake in the short term, particularly among post-abortion patients in Cambodia, but these effects diminished over time. Reis et al. (2019) highlighted similar trends in Bangladesh, where automated voice messages failed to enhance LARC uptake but provided valuable insights into the unintended consequences of mHealth tools, such as increased self-reported intimate partner violence (IPV). These results suggest that while mobile health (mHealth) interventions can address informational gaps, broader systemic barriers, such as limited access to healthcare and sociocultural factors, may hinder their long-term impact.
Studies outside the review further corroborate these findings. For example, Free et al. (2013) emphasised that mHealth interventions improve health knowledge but are less effective when social determinants, such as poverty and education, are not addressed. Similarly, Guse et al. (2012) noted that digital health tools perform well in raising awareness but often lack the infrastructure to support sustained behavioural change in LICs. Additionally, research by Mangone, Lebrun, and Muessig (2016) stressed the role of contextual factors, noting that digital solutions require localised adaptation to address cultural and infrastructural challenges effectively.
Impact in High-Income Countries
In high-income countries (HICs), apps like Natural Cycles demonstrated greater consistency in outcomes, with a Pearl Index of 1.0 for perfect use, comparable to oral contraceptives (Scherwitzl et al., 2016, 2017). These apps are particularly appealing to users seeking hormone-free contraceptive options. However, typical-use Pearl Indices of 6.9 highlight the challenge of ensuring user adherence and accurate data entry. These findings underscore the need for improved educational strategies and app designs that promote consistent engagement. Despite these challenges, apps in HICs benefit from higher levels of digital literacy and access to reliable technology, making them a viable alternative for individuals seeking non-hormonal contraceptive methods.
Comparative studies bolster these observations. A trial by Chuang et al. (2015) comparing a web-based reproductive planning intervention to standard care showed higher satisfaction in the intervention group but limited improvements in contraceptive efficacy. This suggests that while digital tools in HICs enhance user autonomy and satisfaction, integrating professional oversight remains critical for optimising outcomes. Moreover, Raymond et al. (2019) highlighted the effectiveness of telehealth platforms like TelAbortion in providing remote, professional reproductive care, underscoring the complementary role that mobile apps could play alongside such services.
User Engagement and Retention
One of the most significant challenges identified across all settings was the variability in user engagement. High dropout rates, as reported by Scherwitzl et al. (2016), suggest that users often disengage due to dissatisfaction with app interfaces, a perceived complexity in navigation, or a lack of tangible benefits from using the tools. McCarthy et al. (2019) observed similar challenges in Palestine, where despite an improvement in contraceptive acceptability rates, there was no significant increase in actual contraceptive use among participants. To address these issues, incorporating features such as gamification, community support networks, and regular follow-ups could play a pivotal role in mitigating user fatigue and encouraging sustained engagement. Additionally, integrating these apps with telehealth services could significantly enhance retention by offering users direct access to healthcare professionals for personalised guidance and support.
Studies like Smith et al. (2015) further underscore the value of combining digital interventions with counsellor support, which was shown to sustain user engagement and improve outcomes, such as the uptake of long-acting reversible contraception (LARC). Research by Hollander and Carr (2020) reinforces these findings, highlighting the importance of interactive features and user feedback in maintaining long-term engagement. They argue that applications integrated into broader healthcare ecosystems consistently outperform standalone digital tools in terms of user retention and satisfaction. Similarly, a systematic literature review conducted by Kruse et al. (2017) emphasised that digital interventions incorporating personal contact achieve higher engagement rates than those relying solely on technological features, further demonstrating the importance of hybrid approaches to digital healthcare solutions.
Addressing Digital Inequities
The effectiveness of mobile contraceptive applications in low- and middle-income countries (LICs) is significantly constrained by persistent digital inequities. Limited access to smartphones and reliable internet connections, as highlighted by Reis et al. (2019), restricts the reach and impact of these interventions, leaving many potential users underserved. Addressing these disparities requires targeted investments in digital infrastructure to improve connectivity, alongside initiatives aimed at enhancing digital literacy among marginalised populations. Simplified app interfaces designed for ease of use, combined with offline functionality, could play a crucial role in making these tools more accessible and inclusive for users with limited technical skills or intermittent internet access.
Additionally, fostering partnerships with local governments and non-governmental organisations (NGOs) could help to scale these solutions effectively, ensuring that they reach underserved regions and populations. Such collaborations could facilitate broader adoption and promote equitable access to reproductive health services through mobile technologies. Comparative frameworks discussed by Kruse et al. (2017) emphasise the critical role of public-private partnerships in bridging these digital divides. They provide examples of successful initiatives where governments subsidised mobile technologies to expand the reach of health apps in rural and remote areas, offering a viable model for LICs to replicate.
Furthermore, guidelines from the World Health Organization (2016) advocate for integrating mobile health tools into broader public health strategies. These guidelines highlight the importance of sustainable funding models and capacity-building initiatives to ensure the long-term viability and scalability of digital health solutions. By addressing these challenges, mobile contraceptive applications could achieve greater effectiveness and impact in LICs.
Privacy and Security Concerns
The sensitivity of reproductive health data presents significant privacy and security challenges that must be addressed to ensure user trust and widespread adoption of mobile applications. Although not explicitly discussed in all studies reviewed, the implementation of robust data protection mechanisms is essential to safeguard sensitive personal information. Scherwitzl et al. (2016) and McCarthy et al. (2019) underscored the critical role of user education in addressing misconceptions related to app functionality and data handling processes. Developers should priorities the use of strong encryption technologies, the establishment of transparent data policies, and the integration of secure authentication methods to mitigate risks and foster confidence among users. Adopting these measures would ensure that users feel reassured about the secure handling of their data.
Regulatory frameworks, such as the General Data Protection Regulation (GDPR), provide valuable guidance for maintaining compliance and protecting user information. These frameworks help standardize data security practices and establish a foundation of trust. Gómez-Ramírez et al. (2021) further emphasized that user confidence in digital tools is closely linked to transparent communication about how data is used and protected. They recommend periodic audits and the introduction of certification mechanisms as effective ways to reinforce accountability and enhance trust. Comparisons with other fields in health technology suggest that integrating certification processes and adhering to best practices could significantly bolster user trust, ultimately encouraging broader adoption and sustained engagement with reproductive health applications.
Integration with Standard Care
Mobile contraceptive applications should function as complementary tools rather than standalone solutions, effectively integrating with standard healthcare services to maximize their impact and effectiveness. By connecting these applications with broader healthcare systems, such as providing reminders for follow-up visits, offering tailored feedback, or facilitating telemedicine consultations, adherence and user outcomes could be significantly enhanced. Evidence from studies like Smith et al. (2015) demonstrates the value of combining digital interventions with counsellor support, which markedly improved long-acting reversible contraception (LARC) uptake among participants. This highlights the importance of blending human interaction with technological solutions to optimize results.
In Bolivia, McCarthy et al. (2020) suggested that integrating app-based educational interventions with in-person consultations could address persistent gaps in contraceptive use, improving both short-term and sustained impacts. Telemedicine comparisons further underscore this potential. For example, the TelAbortion project (Raymond et al., 2019) demonstrated how telehealth platforms facilitated safe, effective reproductive healthcare services. This success indicates that similar integrations with contraceptive applications could amplify their benefits by combining the convenience of digital tools with the reliability of professional oversight.
Findings align with recommendations from Kruse et al. (2017), who advocate for hybrid models that merge technological innovation with direct human support to optimize care delivery and user satisfaction. Free et al. (2013) similarly highlighted how integrating mHealth tools with traditional healthcare services can effectively address systemic barriers and improve long-term outcomes. These hybrid approaches ensure that mobile applications enhance, rather than replace, the quality and accessibility of reproductive health services.
Future Directions
The potential of mobile contraceptive applications can be fully realized through strategic enhancements. The integration of adaptive algorithms into fertility-awareness-based methods represents a promising avenue for improving predictive accuracy by accounting for individual variability and external influences, including psychosocial stress and intercurrent illness. Such advancements could address longstanding limitations in reliability and usability, thereby enhancing the effectiveness of these tools in both clinical and real-world contexts. Beyond algorithmic refinements, the incorporation of community engagement features—such as interactive peer forums and structured opportunities for counsellor interaction—may provide critical psychosocial benefits. Existing evidence suggests that peer support and professional guidance can mitigate disengagement, foster a sense of belonging, and sustain adherence to digital health interventions over time.
Expanding the scope of mobile applications to encompass a broader range of reproductive health functionalities, including menstrual cycle monitoring, fertility planning, and comprehensive educational resources on sexually transmitted infections, preventive care, and overall reproductive health, aligns with a more holistic, user-centred approach. Such diversification of functions may improve reproductive health literacy and promote informed decision-making, with potential downstream effects on reproductive outcomes and general health. Equally important is the imperative to strengthen accessibility, particularly in underserved or resource-limited settings. User interface simplification, multilingual support, and offline functionality are practical measures to reduce barriers related to digital literacy and connectivity, while collaborations with technology providers, NGOs, and community organisations may play a pivotal role in reducing inequities in access and utilisation.
Finally, safeguarding user trust remains central to the sustainable adoption of digital reproductive health applications. Transparent data governance, robust encryption, and compliance with international data protection frameworks are critical for ensuring the confidentiality and security of sensitive personal information. From a research perspective, future studies should not only evaluate the clinical effectiveness of these applications but also systematically examine user engagement, accessibility, and data security as mediating factors influencing adoption and long-term outcomes.
Long-Term Research Needs
Future research should explore the long-term impacts of mobile contraceptive applications, particularly in low- and middle-income countries (LICs) where systemic barriers such as digital inequities, cultural norms, and limited healthcare infrastructure may restrict their effectiveness. Understanding the sustained engagement patterns of users over extended periods is essential to determine whether these tools can meaningfully influence contraceptive use, unintended pregnancy rates, and broader reproductive health outcomes. Longitudinal studies could provide critical insights into how users interact with these applications over time, including factors that enhance or diminish engagement and adherence.
Additionally, comparative studies are needed to evaluate the effectiveness of mobile applications when integrated with telehealth services and traditional care models. For example, research could assess whether app-based interventions combined with in-person counselling or telemedicine consultations improve outcomes more effectively than standalone apps. Further investigation into user demographics, such as age, education level, and digital literacy, would help tailor interventions to diverse populations, ensuring equitable access and impact.
Expanding research to include qualitative studies could also illuminate user experiences, highlighting barriers to sustained use and opportunities for enhancing functionality. By addressing these gaps, future studies can inform the design of more effective, inclusive, and impactful mHealth solutions for contraceptive care worldwide.
Limitations of Contraceptive Applications
Digital Literacy and Access
Limited digital literacy and access to technology emerged as significant barriers, particularly in low- and middle-income countries (LMICs). McCarthy et al. (2018, 2020) highlighted persistent challenges in Tajikistan and Bolivia, where issues such as under-recruitment and low intervention doses negatively affected the outcomes of mobile health interventions. Similarly, Reis et al. (2019) identified critical infrastructure gaps in Bangladesh, which significantly hindered the broader adoption and effective implementation of mHealth tools in the region. These persistent barriers strongly underscore the urgent need for targeted initiatives aimed at improving digital inclusivity through simplified mobile application designs and comprehensive, targeted training programs for users.
Privacy and Security Concerns
Concerns regarding privacy and data security were a significant underlying issue in studies that utilised mobile platforms to collect sensitive reproductive health data. While these concerns were not explicitly addressed in most of the reviewed studies, their importance cannot be overstated. User trust is a critical factor in ensuring engagement with mobile health interventions, particularly in sensitive areas like reproductive health. Without adequate safeguards, users may hesitate to provide accurate information or fully participate in such programs. To address these issues, developers must prioritise implementing robust encryption methods to protect data during transmission and storage. Additionally, transparent data policies, including clear terms of use and consent agreements, are essential to reassure users about how their information will be handled. Proactively addressing privacy concerns can enhance trust and promote broader adoption of mobile health platforms
User Engagement Variability
Engagement variability clearly emerged as a key limitation across the studies reviewed. Scherwitzl et al. (2016, 2017) reported significantly high discontinuation rates of 54.6%, primarily attributed to user dissatisfaction and inconsistent use of fertility-awareness-based mobile applications. In Cambodia, Smith et al. (2015) observed declining contraceptive uptake over time, even though there was initial success in improving usage rates shortly after intervention. These findings collectively highlight the critical importance of addressing user fatigue, which often leads to disengagement and enhancing the interactivity of mobile health tools to better sustain user engagement and promote long-term adherence to these digital interventions.
Effectiveness Variability
Variability in effectiveness was clearly evident across the studies reviewed, and it was often linked to user-dependent factors. Scherwitzl et al. (2016, 2017) demonstrated notable disparities between typical use and perfect use of contraceptive mobile applications, thereby emphasising the significant impact of adherence on outcomes. Reis et al. (2019), on the other hand, found that external factors, such as incidents of intimate partner violence (IPV), can undermine the overall success of such interventions. These combined results strongly suggest that mHealth tools must incorporate advanced adaptive algorithms and provide contextual support to enhance reliability, improve user engagement, and better address individual needs.
Strengths and Limitations of the Study
The study demonstrates several notable strengths, including its comprehensive scope and rigorous methodology. By systematically reviewing contraceptive mobile applications across diverse global settings, it captures a broad range of user demographics, cultural contexts, and health outcomes, ensuring relevance to both high-income and low-income country contexts. The use of established and widely accepted frameworks, such as PRISMA guidelines, alongside robust quality assessment tools like the Cochrane Risk of Bias and Newcastle-Ottawa Scale, significantly adds to the credibility and reliability of the findings. Additionally, the inclusion of both randomised controlled trials and observational studies provides a well-rounded perspective, balancing evidence from controlled experimental conditions with real-world applications. The study's dual focus on primary outcomes, such as unintended pregnancy rates, and secondary measures, like user engagement and adherence, further enriches its analytical depth and practical implications.
However, the study also has several limitations that should be considered. The heterogeneity of the included studies, particularly in terms of their designs, sample populations, and outcome measures, precluded the possibility of conducting a meta-analysis, thereby limiting the ability to synthesise quantitative findings. Moreover, the follow-up periods in most studies were relatively short, restricting the ability to derive insights into the long-term effects and sustainability of mobile contraceptive interventions. While the study acknowledges privacy concerns, it does not thoroughly explore the critical issue of data security, which is essential for building and maintaining user trust. Engagement challenges, such as high dropout rates and inconsistent user participation, emerged as recurring issues that undermine the sustained effectiveness of the interventions. Additionally, the exclusion of non-English studies may have introduced a language bias, potentially omitting relevant data from non-English-speaking regions and limiting the generalizability of the findings. These limitations collectively suggest valuable areas for future research to refine and enhance the understanding, implementation, and effectiveness of mobile contraceptive applications globally.
Conclusion
In conclusion, mobile contraceptive applications show considerable promise in improving reproductive health literacy, contraceptive acceptability, and access to care across diverse settings. While evidence supports their potential effectiveness, challenges related to user adherence, digital inequities, and data privacy limit their broader impact. Addressing these barriers through improved design, stronger privacy safeguards, and integration within comprehensive healthcare systems will be essential for ensuring sustained engagement and achieving meaningful reductions in unintended pregnancies worldwide.
References
- American College of Obstetricians and Gynecologists. (2021). Effectiveness of birth control methods. ACOG.
Publisher | Google Scholor - Berglund Scherwitzl, E., Gemzell Danielsson, K., Sellberg, J. A., & Scherwitzl, R. (2016). Fertility awareness-based mobile application for contraception. The European Journal of Contraception & Reproductive Health Care, 21(3):234–241.
Publisher | Google Scholor - Berglund Scherwitzl, E., Lundberg, O., Kopp Kallner, H., Gemzell Danielsson, K., Trussell, J., & Scherwitzl, R. (2017a). Perfect-use and typical-use Pearl Index of a contraceptive mobile app. Contraception, 96(6):420–425.
Publisher | Google Scholor - Berglund Scherwitzl, E., Lundberg, O., Kopp Kallner, H., Gemzell Danielsson, K., Trussell, J., & Scherwitzl, R. (2017b). Perfect-use and typical-use Pearl Index of a contraceptive mobile app. Contraception, 96(6):420–425.
Publisher | Google Scholor - Comfort, A. B., Rao, L., Goodman, S., Raine-Bennett, T., Barney, A., Mengesha, et al. (2022). Assessing differences in contraceptive provision through telemedicine among reproductive health providers during the COVID-19 pandemic in the United States. Reproductive Health, 19(1):99.
Publisher | Google Scholor - Duane, M., Contreras, A., Jensen, E. T., & White, A. (2016). The performance of fertility awareness-based method apps marketed to avoid pregnancy. The Journal of the American Board of Family Medicine, 29(4):508–511.
Publisher | Google Scholor - Free, C., Phillips, G., Galli, L., Watson, L., Felix, L., et al. (2013). The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: A systematic literature search and review. PLoS Medicine, 10(1):e1001362.
Publisher | Google Scholor - Gómez-Ramírez, O., Iyamu, I., Ablona, A., Watt, S., Xu, A. X. T., et al. (2021). On the imperative of thinking through the ethical, health equity, and social justice possibilities and limits of digital technologies in public health. Canadian Journal of Public Health, 112(3):412–416.
Publisher | Google Scholor - Guse, K., Levine, D., Martins, S., Lira, A., Gaarde, J., et al. (2012). Interventions using new digital media to improve adolescent sexual health: A systematic literature search and review. Journal of Adolescent Health, 51(6):535–543.
Publisher | Google Scholor - Hebert, L. E., Hill, B. J., Quinn, M., Holl, J. L., Whitaker, A. K., & Gilliam, M. L. (2018). Mobile contraceptive application use in a clinical setting in addition to standard contraceptive counselling: A randomized controlled trial. Contraception, 98(4):281–287.
Publisher | Google Scholor - Hollander, J. E., & Carr, B. G. (2020). Virtually perfect? Telemedicine for Covid-19. New England Journal of Medicine, 382(18):1679–1681.
Publisher | Google Scholor - Kruse, C. S., Krowski, N., Rodriguez, B., Tran, L., Vela, J., & Brooks, M. (2017). Telehealth and patient satisfaction: A systematic literature search and review and narrative analysis. BMJ Open, 7(8):e016242.
Publisher | Google Scholor - Mangone, E. R., Lebrun, V., & Muessig, K. E. (2016). Mobile phone apps for the prevention of unintended pregnancy: A systematic literature search and review and content analysis. JMIR mHealth and uHealth, 4(1):e6.
Publisher | Google Scholor - McCarthy, O., Ahamed, I., Kulaeva, F., Tokhirov, R., Saibov, S., et al. (2018). A randomized controlled trial of an intervention delivered by mobile phone app instant messaging to increase the acceptability of effective contraception among young people in Tajikistan. Reproductive Health, 15(1):28.
Publisher | Google Scholor - McCarthy, O. L., Aliaga, C., Torrico Palacios, M. E., López Gallardo, et al. (2020). An intervention delivered by mobile phone instant messaging to increase acceptability and use of effective contraception among young women in Bolivia: Randomized controlled trial. Journal of Medical Internet Research, 22(6):e14073.
Publisher | Google Scholor - McCarthy, O. L., Zghayyer, H., Stavridis, A., Adada, S., Ahamed, I., et al. (2019). A randomized controlled trial of an intervention delivered by mobile phone text message to increase the acceptability of effective contraception among young women in Palestine. Trials, 20(1):228.
Publisher | Google Scholor - Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic literature search and reviews. BMJ:n71.
Publisher | Google Scholor - Raymond, E., Chong, E., Winikoff, B., Platais, I., Mary, M., Lotarevich, T., et al. (2019). TelAbortion: Evaluation of a direct to patient telemedicine abortion service in the United States. Contraception, 100(3):173–177.
Publisher | Google Scholor - Reiss, K., Andersen, K., Pearson, E., Biswas, K., Taleb, F., Ngo, T. D., et al. (2019). Unintended consequences of mHealth interactive voice messages promoting contraceptive use after menstrual regulation in Bangladesh: Intimate partner violence results from a randomized controlled trial. Global Health: Science and Practice, 7(3):386–403.
Publisher | Google Scholor - Smith, C., Ngo, T. D., Gold, J., Edwards, P., Vannak, U., et al. (2015). Effect of a mobile phone-based intervention on post-abortion contraception: A randomized controlled trial in Cambodia. Bulletin of the World Health Organization, 93(12):842–850A.
Publisher | Google Scholor - Stifani, B. M., Smith, A., Avila, K., Boos, E. W., Ng, J., Levi, et al. (2021). Telemedicine for contraceptive counselling: Patient experiences during the early phase of the COVID-19 pandemic in New York City. Contraception, 104(3):254–261.
Publisher | Google Scholor - United Nations. (2015). Sustainable Development Goals. UN.
Publisher | Google Scholor - United Nations Population Fund. (2022). Nearly half of all pregnancies are unintended—A global crisis. UNFPA.
Publisher | Google Scholor - Winner, B., Peipert, J. F., Zhao, Q., Buckel, C., Madden, T., et al. (2012). Effectiveness of long-acting reversible contraception. New England Journal of Medicine, 366(21):1998–2007.
Publisher | Google Scholor - World Health Organization. (2016). mHealth: Use of mobile wireless technologies for health.
Publisher | Google Scholor - World Health Organization. (2021). Abortion. WHO.
Publisher | Google Scholor























