

Research Article
A Novel Four-Target Microsurgical Approach İn Psychosurgery for Refractory Complex Psychiatric Disorders
1 Department of Neurosurgery, Kafkas Univercity, Kars, Turkey.
2 Department of Neurosurgery, Yenimahalle Training and Research Hospital, University of Yıldırım Beyazıt, Ankara, Turkey.
3 Department of Psychiatry, Private Clinic, Ankara, Turkey.
4 Department of Neurosurgery and Anatomy, Private Clinic, Ankara, Turkey.
*Corresponding Author: Kadir Yıldırım,1Department of Neurosurgery, Kafkas Univercity, Kars, Turkey.
Citation: Yıldırım K, Coşar A, Analan E, Mehmet E Üstün. (2026). A Novel Four-Target Microsurgical Approach İn Psychosurgery for Refractory Complex Psychiatric Disorders. Journal of Neuroscience and Neurological Research. BioRes Scientia Publishers. 5(1):1-6. DOI: 10.59657/2837-4843.brs.26.040
Copyright: © 2026 Kadir Yıldırım, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 22, 2026 | Accepted: February 23, 2026 | Published: March 02, 2026
Abstract
Background: Psychosurgery remains a therapeutic option for a small subset of patients with severe psychiatric disorders who are refractory to pharmacological treatment, psychotherapy, and electroconvulsive therapy, particularly in the presence of persistent suicidality or severe behavioral dysregulation. Conventional psychosurgical procedures generally target one or two limbic structures, which may be insufficient in patients with complex multi-psychiatric conditions.
Methods: We retrospectively analyzed nine patients with long-standing, treatment-resistant psychiatric disorders who underwent a novel microsurgical psychosurgical procedure between 2018 and 2024. The technique involves a single parasagittal frontal mini-craniotomy allowing access to four distinct targets: bilateral cingulate gyrus, bilateral subcaudate region, bilateral stria terminalis, and the genu of the corpus callosum. Postoperative clinical assessments were conducted at 1, 3, 6, and 12 months by an independent multidisciplinary team.
Results: No mortality or permanent neurological morbidity was observed. Clinically meaningful improvement in psychiatric symptoms was noted in all patients. Within the first postoperative month, 7 of 9 patients (78%) required substantial reduction of psychiatric medications. By the third postoperative month, most patients had discontinued pharmacological treatment under psychiatric supervision. Two patients (22%) required a single medication until the sixth month, which was subsequently discontinued. Improvements were particularly notable in aggression, impulsivity, and suicidal ideation.
Conclusion: This technical report introduces a novel four-target microsurgical approach designed to address complex neural circuits implicated in refractory multi-psychiatric disorders. Preliminary results suggest that simultaneous modulation of multiple limbic and interhemispheric pathways may enhance clinical outcomes compared with conventional psychosurgical techniques. Further studies with larger cohorts are warranted to validate these findings.
Keywords: psychosurgery; cingulotomy; subcaudate tractotomy; stria terminalis; callosotomy; limbic leucotomy; refractory psychiatric disorders
Introduction
Psychosurgery was introduced in 1935 with the first frontal lobotomy performed by Moniz, marking the beginning of surgical intervention for psychiatric disease [1]. Although early procedures were associated with significant morbidity, subsequent decades saw the refinement of targets and techniques, particularly with the introduction of stereotactic methods aimed at improving precision and safety [2,3]. The cingulate gyrus, subcaudate region, and anterior limb of the internal capsule gradually emerged as principal targets for major depressive disorder, obsessive–compulsive disorder, panic disorder, and phobias [4–6].
Despite major advances in pharmacological and psychotherapeutic strategies, approximately 10–20% of patients with severe psychiatric disorders remain refractory to standard treatments, often presenting with persistent suicidality, aggression, or profound behavioral dysregulation [7–9]. In such cases, psychosurgery continues to be considered as a last-resort therapeutic option. However, conventional psychosurgical procedures typically involve lesioning one or two bilateral targets, which may be insufficient to modulate the complex and distributed neural networks underlying multi-psychiatric conditions [10,11].
Limbic leucotomy, combining cingulotomy and subcaudate tractotomy, represents a well-established approach for treatment-resistant cases [12]. Transection of the stria terminalis, functionally analogous to amygdalotomy, has been associated with improved control of aggression and impulsivity [13,14]. Additionally, growing neuroimaging evidence has demonstrated structural and functional abnormalities of the corpus callosum—particularly the genu—in schizophrenia, bipolar disorder, and schizoaffective disorder, implicating interhemispheric dysconnectivity in disease pathophysiology [15–18]. These findings support the rationale for a multi-target approach aimed at simultaneously modulating interconnected limbic and interhemispheric circuits in patients with refractory, complex psychiatric disorders.
Methods
Study Design and Patients
This retrospective study included nine patients who underwent the described psychosurgical procedure between 2018 and 2024. All patients had a documented history of treatment resistance lasting 5–15 years despite optimal pharmacotherapy, psychotherapy, and electroconvulsive therapy. Persistent suicidality, aggression, or severe impulsivity were present in all cases, while 1 patient had catatonic schizophrenia, 4 patients had bipolar disorder, and 4 patients had schizoaffective disorder (Table-1).
Table 1: Disease Distribution of Surgically Treated Patients
| Multiple Diagn | 1 | Aggressivity and Impulsivity (Impulse Control and Behavioral Disorders) | ||
| 2 | Bipolar Disorder | Schizoaffective Disorder | Catatonic Schizophrenia | |
| Number of Patients | 4 | 4 | 1 | |
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee (Protocol No: 592, Date: 10.02.2025). Written informed consent was obtained from all patients or their legal representatives.
Clinical Evaluation
Postoperative evaluations were performed at 1, 3, 6, and 12 months by an independent multidisciplinary team consisting of a neurosurgeon, psychiatrist, and psychologist. Clinical improvement was assessed based on symptom severity, behavioral control, and medication requirements.
Surgical Technique
Intraoperative neuromonitoring was used throughout the procedure (Figure.1-A). All four targets lie along the same parasagittal plane but at different depths, allowing access through a single parasagittal frontal mini-craniotomy measuring approximately 3 × 3 cm (Figure.1-B). Using an anterior interhemispheric microsurgical approach, (Figure.2) the following procedures were performed: bilateral cingulotomy (Figure.3-A), transection of the genu of the corpus callosum (Figure.3-B), bilateral subcaudate tractotomy (Figure.3-C), and bilateral transection of the stria terminalis (Figure.3-D). The sequence of target modulation was determined based on anatomical depth and surgical exposure.

Figure 1A: Shows the position of the patient with neuromonitorization
Figure 1B: Shows the dimensions of the mini craniotomy

Figure 2: Shows anterior interhemispheric approach after a parasagittal frontal mini craniotomy.
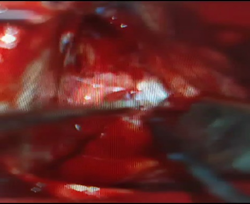
Figure 3A: Shows the intraoperative view of cingulotomy.

Figure 3B: Shows the intraoperative view of callosotomy

Figure 3C: Shows the intraoperative view of subcaudate tractotomy.

Figure 3D: Shows the incision of the stria terminalis intraoperatively
Results
All procedures were completed without intraoperative complications. No patient experienced mortality, permanent neurological deficit, or significant postoperative morbidity. Clinical improvement was observed in all patients. Within one month postoperatively, 78% of patients required significant reduction of psychiatric medications. By the third month, the majority had discontinued pharmacological treatment entirely. Two patients continued a single medication until the sixth month, after which pharmacotherapy was discontinued under psychiatric supervision. Marked reductions in aggression, impulsivity, and suicidal ideation were consistently observed.
Discussion
The present technical report proposes a four-target microsurgical approach designed to address the limitations of conventional psychosurgical techniques. By simultaneously targeting multiple nodes within the limbic and interhemispheric networks, this strategy seeks to achieve broader circuit modulation than single- or dual-target procedures [11,12,19]. Previous studies have shown that isolated lesioning of the cingulate gyrus or subcaudate region can result in partial or delayed clinical responses, particularly in patients with comorbid psychiatric diagnoses [6,10]. Similarly, amygdalotomy or stria terminalis transection alone may be insufficient to control complex behavioral dysregulation when higher-order frontal–limbic connectivity remains intact [13,14]. The inclusion of anterior callosotomy in the present approach is supported by evidence linking corpus callosum abnormalities to impaired emotional regulation, aggression, and psychotic symptoms [16–18,20].
Although the small sample size and retrospective design limit definitive conclusions, the favorable safety profile and consistent clinical improvements observed in this series align with previous reports advocating multi-target psychosurgical strategies in carefully selected patients [19–21]. Prospective studies incorporating standardized psychiatric outcome measures and neuroimaging correlates are required to further elucidate the mechanisms and long-term efficacy of this approach. This novel microsurgical psychosurgical technique represents a promising approach for carefully selected patients with refractory multi-psychiatric disorders. The favorable safety profile and encouraging clinical outcomes observed in this preliminary series warrant further investigation in larger, controlled studies.
Limitations
The primary limitations of this study include the small sample size, retrospective design, and lack of a control group. Additionally, formal standardized psychiatric rating scales were not uniformly applied. These factors limit the generalizability of the findings and underscore the need for prospective studies.
Declarations
Ethics approval and consent to participate
Approved by the institutional ethics committee (Protocol No: 592, Date: 10.02.2025). Written informed consent was obtained.
Consent for publication
Obtained from all participants or their legal representatives.
Availability of data and materials
Data are available from the corresponding author upon reasonable request.
Competing interests
The authors declare no competing interests.
Funding
This research received no specific grant from any funding agency.
Authors’ contributions
Research conception and design: Kadir Yıldırım, Enver Analan, Aymer Coşar, Mehmet Erkan Üstün.
Data acquisition: Kadir Yıldırım, Enver Analan, Aymer Coşar, Mehmet Erkan Üstün Statistical analysis: Kadir Yıldırım, Enver Analan, Aymer Coşar, Mehmet Erkan Üstün Data analysis and interpretation: Kadir Yıldırım, Enver Analan, Aymer Coşar, Mehmet Erkan Üstün.
Drafting of the manuscript: Kadir Yıldırım, Enver Analan, Aymer Coşar, Mehmet Erkan Üstün Critical revision of the manuscript: Kadir Yıldırım, Mehmet Erkan Üstün Supervision: Kadir Yıldırım, Mehmet Erkan Üstün.
Conflicts of interest
Authors have no conflicts of interest. The authors have nothing to disclose.
Ethical Statement
Our study was approved by the Ethics Committee on 10/02/2025 (80576354-050-99/664). All ethical rules in the Declaration of Helsinki were complied with
References
- Mashour GA, Walker EE, Martuza RL.(2004). Psychosurgery: past, present, and future. Brain Res Rev. 2005;48(3):409-419.
Publisher | Google Scholor - Moniz E.(1937). Prefrontal leucotomy in the treatment of mental disorders. Am J Psychiatry;93(6):1379-1385.
Publisher | Google Scholor - Leksell L.(1951). The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. ;102(4):316-319.
Publisher | Google Scholor - Greenberg BD, Rauch SL, Haber SN.(2010). Invasive circuitry-based neurotherapeutics: stereotactic ablation and deep brain stimulation for major depressive disorder. Neuropsychopharmacology.35(1):317-336.
Publisher | Google Scholor - Hurwitz TA, Honey CR, Michell W, et al.,(2024). Ventral targeted anterior capsulotomy for treatment-resistant depression and obsessive–compulsive disorder. Psychiatry Res.,333:115435.
Publisher | Google Scholor - Kelly D, Richardson A, Mitchell-Heggs N.(1973). Stereotactic limbic leucotomy: neurophysiological aspects and operative technique. Br J Psychiatry.123(573):133-140.
Publisher | Google Scholor - Lapidus KAB, Saha AR, Heller AC, Blumberger DM, Lozano AM.(2013). History of psychosurgery: a psychiatrist’s perspective. World Neurosurg.,80(3-4):S27.e1-S27.e16.
Publisher | Google Scholor - Da Costa DA.(1997). The role of psychosurgery in selected cases of refractory schizophrenia: a reappraisal. Schizophr Res.,28(2-3):223-230.
Publisher | Google Scholor - Dickerson FB.(2000). Cognitive behavioral psychotherapy for schizophrenia: a review of recent empirical studies. J Nerv Ment Dis.,188(3):187-201.
Publisher | Google Scholor - Gupta R, Graffeo CS, Abraham P, et al.(2024). Benefits of stereotactic radiosurgical anterior capsulotomy for treatment-refractory obsessive-compulsive disorder. J Neurosurg.,141(2):394-403.
Publisher | Google Scholor - Cox AW, Brown MH.(1977). Results of multi-target limbic surgery in the treatment of schizophrenia and aggressive states. In: Sweet WH, Obrador S, Martin-Rodriguez JG, eds. Neurosurgical Treatment in Psychiatry, Pain and Epilepsy:469-482.
Publisher | Google Scholor - Vilela-Filho O, Ragazzo PC, Canêdo D, et al.(2021). The impact of subcaudate tractotomy on delusions and hallucinations in psychotic patients. Surg Neurol Int.,12:475.
Publisher | Google Scholor - Vilela-Filho O.(2019). Commentary: Amygdala and hypothalamus—historical overview with a focus on aggression. Neurosurgery,85(1):E1-E3.
Publisher | Google Scholor - Sano K, Sekino H.(1964).Anterior cingulotomy and amygdalotomy. Confin Neurol.,24:289-301.
Publisher | Google Scholor - Price G, Cercignani M, Parker GJM, et al.(2007). Abnormal brain connectivity in first-episode psychosis: a diffusion MRI tractography study of the corpus callosum. Neuroimage,35(2):458-466.
Publisher | Google Scholor - Brambilla P, Nicoletti MA, Sassi RB, et al.(2003). Magnetic resonance imaging study of corpus callosum abnormalities in bipolar disorder. Biol Psychiatry,54(12):1294-1297.
Publisher | Google Scholor - Brambilla P, Nicoletti M, Sassi RB, et al.(2004). Corpus callosum signal intensity in bipolar and unipolar disorder. J Neurol Neurosurg Psychiatry,75(2):221-225.
Publisher | Google Scholor - Brambilla P, Cerini R, Gasparini A, et al.(2005). Investigation of corpus callosum in schizophrenia with diffusion imaging. Schizophr Res.,79(2-3):201-210.
Publisher | Google Scholor - Greenberg BD, Rezai AR.(2008). Neurotherapeutic interventions for refractory psychiatric disease. CNS Spectr.,13(3):196-204.
Publisher | Google Scholor - Van den Heuvel MP, Hulshoff Pol HE.(2010). Exploring the brain network: a review on resting-state fMRI functional connectivity. Nat Rev Neurosci.,11(3):157-169.
Publisher | Google Scholor - American Psychiatric Association.(1994). Diagnostic and Statistical Manual of Mental Disorders. 4th ed. American Psychiatric Association.
Publisher | Google Scholor























